
Something that is often forgotten by people who are trying to stimulate the pituitary gland to release excess human growth hormone for height increase and to grow taller is that the pituitary gland is not the actual real originator of the hormone pathway. It is the hypothalamus which controls how much somatotropin will be allowed to be released by the pituitary gland.
From source, we find out what are the types of hormones the hypothalamus will released…
The hypothalamus is a region of the brain . It contains several types of neurons responsible for secreting different hormones.
- Thyrotropin-releasing hormone (TRH)
- Gonadotropin-releasing hormone (GnRH)
- Growth hormone-releasing hormone (GHRH)
- Corticotropin-releasing hormone (CRH)
- Somatostatin
- Dopamine
All of these are released into the blood in the capillaries and travel immediately – in portal veins – to a second capillary bed in the anterior lobe of the pituitary, where they exert their effects.
All of them are released in periodic spurts. In fact, replacement hormone therapy with these hormones does not work unless the replacements are also given in spurts.
Two other hypothalamic hormones are vasopressin and oxytocin which travel in the neurons themselves to the posterior lobe of the pituitary where they are released into the circulation.
It would go slightly more detailed on the effects of the Growth hormone-releasing hormone (GHRH)..
Growth Hormone-releasing Hormone (GHRH): GHRH is a mixture of two peptides, one containing 40 amino acids, the other 44. As its name indicates, GHRH stimulates cells in the anterior lobe of the pituitary to secrete growth hormone (GH).
There is also the fact that the hypothalamus will be releasing another hormone which will have an ibhibitory effect on the pituitaty gland in regulating the excess release of growth hormone.
Somatostatin: Somatostatin is a mixture of two peptides, one of 14 amino acids, the other of 28. Somatostatin acts on the anterior lobe of the pituitary to…
- inhibit the release of growth hormone (GH)
- inhibit the release of thyroid-stimulating hormone (TSH)
Somatostatin is also secreted by cells in the pancreas and in the intestine where it inhibits the secretion of a variety of other hormones.
Now, there are at least 8 of these hormones the hypothalamus will be in control of regulating. We will only focus on the Somatostatin and the Growth Hormone-releasing Hormone because they are most relevant to any possible ideas on figuring out how to induce or increase longitudinal growth.
Things like gonadotropin releasing hormone, dopamine, vasopressin, and oxytocin are related to the onset bodily signs of puberty and the regulation of moods and emotions, at least from what we remember from those commercials on TV. As for thyrotropin-releasing hormone and corticotropin-releasing hormone I know every little except that the corticotropin-releasing hormone is released as a response to stress and that corticosteroids are increased.
In our past posts that we had spend a little bit of time looking at the pathways and mechanisms on how the pituitary gland affects the other glands in the endocrine system like the adrenal glands.
From the Wikipedia article on Growth Hormone-releasing Hormone,
Growth-hormone-releasing hormone (GHRH), also known as growth-hormone-releasing factor (GRF, GHRF), somatoliberin or somatocrinin, is a releasing hormone for growth hormone. It is a 44 – amino acid peptide hormone produced in the arcuate nucleus of the hypothalamus.
GHRH is released from neurosecretory nerve terminals of these arcuate neurons, and is carried by the hypothalamo-hypophyseal portal system to the anterior pituitary gland where it stimulates growth hormone (GH) secretion by stimulating the growth hormone-releasing hormone receptor. GHRH is released in a pulsatile manner, stimulating similar pulsatile release of GH. In addition, GHRH also promotes slow-wave sleep directly. Growth hormone is required for normal postnatal growth, bone growth, regulatory effects on protein, carbohydrate, and lipid metabolism.
Effect
GHRH stimulates GH production and release by binding to the GHRH Receptor (GHRHR) on cells in the anterior pituitary.
Analysis & Interpretation:
 We can say that the growth hormone releasing hormone seems to be pulsing at a similar rate as the growth hormone itself. What I wonder is whether stimulation of the hypothalamus indirectly will be able to cause excess release of the growth hormone releasing hormone but be able to inhibit the release of somatostatin.
We can say that the growth hormone releasing hormone seems to be pulsing at a similar rate as the growth hormone itself. What I wonder is whether stimulation of the hypothalamus indirectly will be able to cause excess release of the growth hormone releasing hormone but be able to inhibit the release of somatostatin.
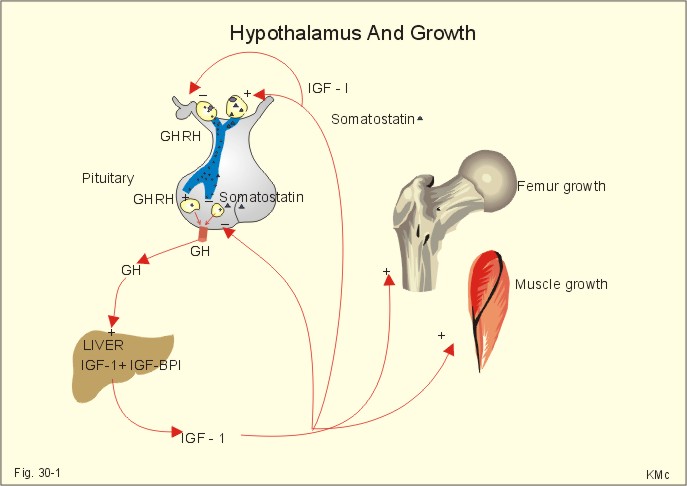
Note: We have already gone over this diagram and well known process many times before in previous posts in the website.
If we can be able to just promote the release of GHRH and prevent also the release of Somatostatin the GH from the pulsating anterior region of the pituitary gland should be able to cause IGF-1 production from the live and also directly effect the growth plates of still developing individuals.
Nature has many ways to prevent organisms from growing out of control so we can see that there is at least two negative feedback loops in the diagram to keep the human body from growing to a crazy size. The IGF-1 produced goes back to increase the amount of somatostatin release by both the hypothalamus and the pituitary gland regions.
If this diagram is a true completed representation of the major routes to possibly increase height in the human body, then we can say that we can block the negative feedback loop process. At this point it could be as simple as putting a filter in the blood vessels that are veins which lead back into the heart and the brain. If we can keep the large sized proteins out of the blood stream then there would not be a signal telling the hypothalamic-pituitary region to stop.
However we did learn that both the GH and the IGF-1 can locally affect the growth plates from a subcetanous incision or injection. The easiest method that physicians have done to promote the increased longitudinal growth of children who have growth hormone defiency is to inject synthetic types of human growth hormone into their arm or shoulder. What I propose that can be simpler is to instead inject IGF-1 and synthetic hGH extremely close to the region of the growth plates. Sure, the old way of injecting so that the hormone will flow throughout the blood and effect all the areas of the body will lead to proportional growth, but if we are focused only on trying to increase our height, it would be smarter then to focus the injections of IGF-1 directly to the growth plate region to gain a higher level of effect. This will be a way to show how we can get around the negative feedback loop of the GHRH/HGH/IGF-1 interactions.
Pingback: Complete List Of Posts - |
Hi My name Michael Anthony I’m DEAF……
36 year old 5’0″1/4 From Hickory, NC USA
I want Tall 6’11” How Much Cost
Is it possible to keep on growing up even after puberty? A 34 year old man could use a stimulation of the hypothalamus ? Increase the production of that HRGR hormone produce in the pituitary gland? Can that be done or is just like a myth?
No. Once your epiphyseal plates close, you are done. There are genetic disorders that cause this to happen very young, usually with an early growth spurt. They can only be treated if caught during latency/puberty.
You got epiphyseal plates once. You can get them again.
Pingback: height growth with hgh releasing hormone - height growth
Theoretically speaking, yes, once the cartilegenous plates fuse, long bone elongation is done but! There is, however, a groundbreaking, albeit very new and very expensive stem cell therapy treatment. It’s still in trial stages but does show some promise.