
Something which I have always guessed could really work in making people grow taller was the use of Extracorporeal Shockwaves. I had written before at least multiple posts about the possibility, showing the dozens of PubMed articles all suggesting that ESW therapy works in bone healing and bone growth, but also the possibility to cause chondrogenesis and chondrocyte proliferation. The post where I wrote about this idea was “New Proposed Height Increase Method Using BMPs And Extracorporeal Shock Wave Treatment, ESWT”
For the Full version of the entire article, click HERE
Title Of Thesis: Non-invasive shock wave stimulated periosteum for bone tissue engineering
Kearney, Cathal (Cathal John) – Harvard University–MIT Division of Health Sciences and Technology.
Thesis (Ph. D.)–Harvard-MIT Division of Health Sciences and Technology, 2011
The cambium cells of the periosteum, which are known osteoprogenitor cells, have limited suitability for clinical applications of bone tissue engineering due to their low cell number (2-5 cells thick). Extracorporeal shock waves (ESWs) have been reported to cause thickening of the cambium layer and subsequent periosteal osteogenesis. This work proposes that ESW-therapy can be used as a non-invasive, inexpensive, and rapid method for stimulating cambium cell proliferation, and investigates the use of these cells for orthotopic bone growth. The response of periosteal cells to ESWs was evaluated using two different energy densities applied to either the intact femur or tibia of the rat. Just four days after application of ESWs, there was a significant 3- to 6-fold increase in cambium cell number and thickness. The most effective treatment of those tested was high dose ESW applied to the tibia. Immunohistochemical staining of the proliferated cells demonstrated osteoblasts and bone formation (osteocalcin stain); it also demonstrated extensive vonWillebrand factor expression, which reveals the vascular contribution to the proliferating cambium layer. In a rabbit model, ESW-thickened cambium layer cells were overlaid in situ on a porous calcium phosphate scaffold. At two weeks post-surgery, there was a significant increase in all outcome variables for the ESW-treated group when compared with controls: a 4-fold increase in osteoprogenitor tissue in the scaffold upper half, a 10- fold increase in osteoprogenitor tissue above the scaffold, and a 2-fold increase in callus size. The results successfully demonstrated the efficacy of ESW-stimulated periosteum for bone tissue engineering.
Analysis & Interpretation:
The thing about Ph. D programs are that they are very long and mentally intensive. What is well known is that for a person to be awarded a degree in graduate school, for say a Masters or Doctorate, they have to do more than just regurgitate the information that is already in the scholarly books, but create something new or answer some question which has not been answered yet. Also, Ph. D. Thesis tend to be more like novels since they are almost always over 100+ pages in length. This means that I will NEVER take that much time in analyzing every single sentence.
However I will explain why this MIT Thesis from 2011 is so important. It shows that we have finally discovered a real way to increase out height noninvasively, through the application of a type of vibration or wave to stimulate cell proliferation in an area of the body which can be stimulated since it still has progenitor mesenchyme-like cells which can differentiate into the type of cells we are looking for.
From my analysis of just the Abstract this is the real deal.
Not only does this show finally the first real to way to increase our height, it also validates one of the primary ideas I have been having, which is that we might be able to manipulate the cambium cells in the lower periosteum layer to grow in thickness from proliferation.
Increased thickness means the end of our long bones in our legs would be thicker, which translate to extra height.
If you are a true researcher, then I would suggest you go through the pages 40-52 where the Ph. D candidate goes into the introduction on the periosteum and the responses to extracorporeal shockwaves. The Thesis has results sections, but I would rather just focus on reading the “discussion” sections to see how the researcher is interpreting the data. I would assume that a person who has managed to make it through the Ph. D program in the hard sciences or engineering from MIT is intelligent enough to read and interpret the data they have received correctly, since they probably have been working on the problem for at least a couple of years.
They state …
“The focus of this thesis is the generation of bone orthotopically using ESW-stimulated periosteum in combination with a subperiosteally implanted porous cal- cium phosphate scaffold. ” (pg. 43 of 225)
This may mean that the person is only doing the research to make bones stronger and have greater bone mass density (BMD) to treat aged people with osteoporosis but it also shows that the results mean that applied the right way a subject can in theory gain a little bit of height increase.
Let’s look at this picture I clipped from page 44 which shows the diagram on how autologous chondrocyte transplant or autologous chondrocyte implantation (ATI) treatment would work.
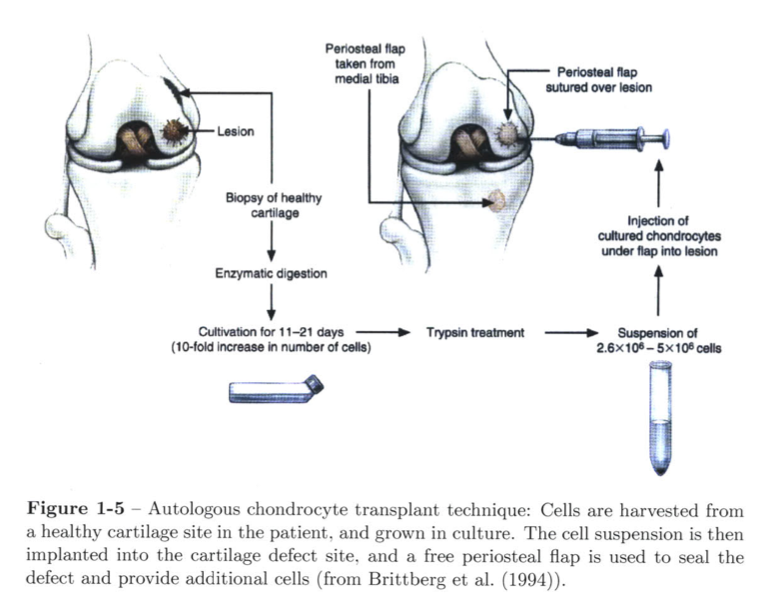
This is how the general implantation is supposed to work. However the technique here is specified for using a periosteal flap for a place to get chondrocytes. in using the periosteum. The rather sucky thing is that this guy did not decide to look at how feasible it would be to use periosteal tissue in cartilage tissue engineering and cartilage regeneration. They focused on bone growth.
From page 45 in the section 1.3.2 entitled “Thickening of Periosteal Cambium Layer”
Thickening of periosteal cambium layer
Previous investigators have reported techniques aimed at thickening the cambium layer of periosteal cells for use in tissue engineering strategies. O’Driscoll’s group injected TGF-#1 subperiosteally to stimulate periosteal proliferation and to initi- ate chondrogenic differentiation of the cambium cells (Reinholz et al., 2009). Simon et al. (2003) investigated the use of surgical techniques to stimulate periosteal cell proliferation in a caprine model. The authors performed surgical release of the pe- riosteum which resulted in cambium cell proliferation and subsequent bone formation within the proliferated layer
From Section 1.4 on Extracorporeal Shockwaves…
Our supposition is to employ extracorporeal shock waves (ESWs) as a non-invasive and rapid way of safely and reliably stimulating the proliferation of the periosteal osteoprogenitor cells for use in orthotopic bone generation strategies after only a few days
We have to clear evidence from at least two studies that the ESW would work in making the bone ends thicker then.
Under Section 1.5 for Thesis Goals….
This thesis deals with a new therapeutic approach for regenerating bone orthotopi- cally. The emphasis is on growing bone on the cortical bone surface, which would have applications in bone regeneration in oral and maxillofacial surgery (e.g., alveolar ridge resorption), as well as in orthopaedics (e.g., osteolysis). The central hypoth- esis is that extracorporeal shock wave (ESW)-stimulated periosteum enhances bone formation in porous biomaterials implanted under the periosteum. The overall goal of this work is to demonstrate the efficacy of an ESW-thickened periosteum as an overlay on a porous calcium phosphate scaffold for the orthotopic growth of bone.
If we just skip to pages 72-75, where the Ph. D Candidate writes in the Discussion and Summary section…
Section 2.4
The objectives of this study were to determine the effects of energy flux density (0.15 vs. 0.40 mJ/mm2) and anatomic location (femur vs. tibia) on the periosteal cambium layer cell number. For all groups evaluated, cambium layer cell counts, and cambium layer thickness, were significantly increased following ESW treatment when compared to controls. The higher dose of ESWs resulted in a thicker periosteum compared to the lower dose (Group 3 vs. Group 4; t-test, p<.0001), which is consistent with previous findings (Tischer et al., 2008). However, the results presented here demonstrate a lower threshold for periosteal proliferation (0.15mJ/mm 2 ) when compared with a previous study that reported a minimum energy density of 0.5mJ/mm 2 was required for periosteal osteogenesis (Tischer et al., 2008). The data presented here show that a lower energy density, which reduces inflammation, can be used to stimulate the cambium cells. Tibial periosteum displayed a greater degree of cellular proliferation in response to ESWs compared to the femur (Group 3 vs. Group 2; t-test, p<.0001; tibia vs. femur). The larger amount of soft tissue surrounding the femur may cause more attenuation of the shock wave than occurs for the tibia.
Conclusion:
From Sections 1 and 2, we have clear evidence that bone growth can rather easily occur from ESW application on the cambium layer of the periosteum. With higher dosages, at least to a energy flux density of 0.40 mJ/mm^2 the cell layer gets thicker. However the even better news is that the threshold for cell proliferation is lower than the results found from previous studies.
Section 3 is more interesting. The graduate student tried to figure out what types of cells are really found in the cambium layer and he says that the layer of tissue has mostly osteoblast-like progenitor cells, which can be labeled as mesenchyme and sort of “stem-like”. The problem for our goals is that the cells seem to favor and almost always take the path of differentiating into the bone cells, not cartilage cells. They note that previous studies seem to see the same thing, that the cambium progenitor mesenchyme go through the process of intramembraneous ossification, not endochondral ossification. When they checked to see if the cells left any Collagen Type II or Type X, suggesting chondrocyte production and chondrocyte hypertrophy, they found none.
For our guesses that the bone formation is from microfractures induced, the candidate says it is not likely, or that it could be periosteal elevation. What is most important is to show that vascularization is almost immediate after ESW treatment, which might explain why differentiation into osteoblasts are the main pathway goal than chondrocytes.
The reason for the vascularization and the intramembraneous ossification seems to be from two new proteins which I am not familiar with called SMAs and vWFs (VonWillebrand factor) which seem to be found a lot from endothelial cells.
This makes the candidate believe that the endothelial cells might be stem-like and multipotent differentiating only into bone cells when the ESW is applied causing vascularization.
At this point, we end Section 3 and the summary, and reach around page 95 of this 225 page Ph. D. I will probably try in a post later to go through this entire Ph. D and explain away the other sections to explain what all the technical jargon implies. The big thing to take away from this post are these two points.
- ESW application even at a lower energy flex density does cause the periosteum to grow more bone from cambium cell thickness increase, which means we will grow taller by a little using this non-invasive method.
- The problem is that the ESW causes osteogeneis but not chondrogenesis, which is what we should really be focusing on to get grow taller by a much larger amount. Osteogenesis might increase our height by 1 cms maximum (a personal guess) but Chondrogenesis could lead to hypertrophy and multiple inches in height increase.
So, it’s possible to enlarge flat bones thickness by Extracorporeal Shock Waves?