This find I have made is one of those studies that really help push our research a little further and can help us understand better other possible ways to stimulate height increase.
 While I was going through an old haunt or old forum I used to frequent, on TheTallestMan.com forum, I would come across a thread that was entitled “The matt mcgrory gigantism?“. In this thread the posters were trying to figure out whether the now deceased Matt McGrory had the traditional type of gigantism that one would find in pituitary giants.
While I was going through an old haunt or old forum I used to frequent, on TheTallestMan.com forum, I would come across a thread that was entitled “The matt mcgrory gigantism?“. In this thread the posters were trying to figure out whether the now deceased Matt McGrory had the traditional type of gigantism that one would find in pituitary giants.
What these guys have found is truly startling in scope and I wanted to share the information that they managed to find.
It would seem that at least 4 giants that have lived in the last century have all been suffering what could possibly be the same type of genetic abnormality. The #1 likely condition that the people on TheTallestMan.com forum suggest is that all 4 men, Matt McGrory, Siah Khan, Zech Devits, and the The Tallest Filipino aka The Tallest Man In the Philippines have been suffering the Proteus Syndrome.
- The profile on Matt McGrory on the TheTallestMan.com can be found HERE.
- The profile on Zech Devits on the TheTallestMan.com can be found HERE
- The profile on Siah Khan Ibn Kashmir Khan on the TheTallestMan.com can be found HERE.
- The forum thread on The Tallest Filipino aka The Tallest Man in the Philippines can be found HERE.
Note: Interestingly, from this article HERE on ABS-CBN News it is suggested that the tallest man in the philippines is someone named Raul Dillo. From sources we find out that Raul Dillo is claimed to be 7′ 3″ tall who played professional basketball in his native country of Philippines on the team San Juan Knights of the MBA. There is a profile on Raul Dillo on TheTallestMan.com HERE. It seems that Raul Dillo, who I would guess is actually the tallest filipino native, suffers from acromegaly.
of the MBA. There is a profile on Raul Dillo on TheTallestMan.com HERE. It seems that Raul Dillo, who I would guess is actually the tallest filipino native, suffers from acromegaly.
Geting back to the original forum thread, what I find is that the people on this forum apparently have a passion on finding giants and documenting them correctly, which is similar to my obsession on height and height increase. The first poster who goes by the name JuanCarlos states…
 “The characteristics I have observed on these three individuals (Mcgrory, Devits and the discussed tallest filipino) are really abnormaly long feets and hands (In comparation of their height.”
“The characteristics I have observed on these three individuals (Mcgrory, Devits and the discussed tallest filipino) are really abnormaly long feets and hands (In comparation of their height.”
So we know that these giants who look even more abnormal than say “normal” giants have even greater disproportion in their body parts. The main arguement on the idea that these giants don’t suffer from the Proteus Syndrome is that proteus syndrome causes Asymmetric Growth. However this argument against Proteus Syndrome was rebutted by a poster named Roger
“Looks like Proteus syndrome is an extremelly variable condition, with great clinical variability, that can produce hypertrophy of tissues and an increase in size (partial giantism), uncontrolled bone, skin growth…”
Roger also notes that Proteus Syndrome has been traditionally associated incorrectly with the condition known as Neurofibromatosis. Now, We could get into a whole other post and discussion on the link between Proteus Syndrome, Neurofibromatosis, and The Elephant Man aka Joseph Carey Merrick (whose name is sometimes mislabeled John Merrick) but we won’t get into that right now.
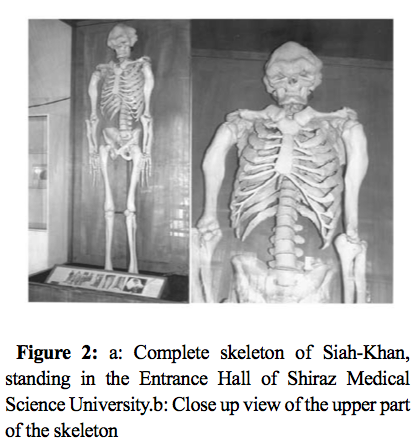
Here are the heights that we know about the giants. Matt McGrory when he was still able to stand without assistance was measured around 7′ 6″. Zech Devits was measured and labeled to be the height of 7′ 8″. Siah Khan was labelled with a height even over 11 feet tall from some sources. However his height was revealed to be around 7′ 2″ due to his extreme vertebrate curvature.
 From that source we find more information about Siah Khan…
From that source we find more information about Siah Khan…
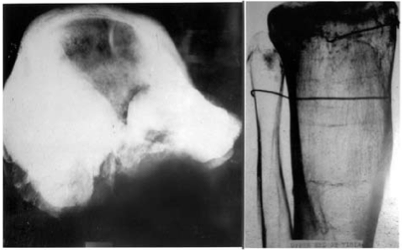
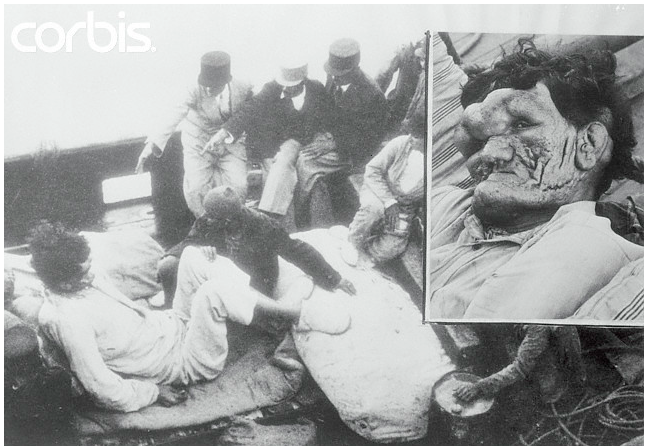
“He clearly had a variety of medical conditions (perhaps one or more of neurofibromatosis, proteus syndrome or elephantiasis) in addition to acromegaly contributing to his physical and mental state. His hands were 117 centimeters long and his legs were 125 centimeters. Siah Khan’s skull weighed 5.7 kilograms but only had a capacity of 1,470 cubic centimeters. As a result of his complicated growth, there was no space in between the vertebrae in his vertebral column.”
“His forehead initially expanded forward and gradually also extended downwards partially covering his eyes. His chin also protruded forward in a sharp manner….. The weight of his head and skull caused him to slouch like a hunchback (without the slouching his height would have been even more).”
It would be Roger in a subsequent post which would make me see something new. He states in a post (He is referring to a picture on the link HERE)…
“Personally, I think the resemblance between this boy affected with Proteus syndrome, and McGrory, Devits and the filipino man is impressive: big ears, protruding forehead, kyphoscoliosis, retrognatia, slim limbs, knee ankylosis, hemihypertrophy of one side of the body (hence, their sloping to one side), etc. The only feature that they do not show is the macrodactyly.”
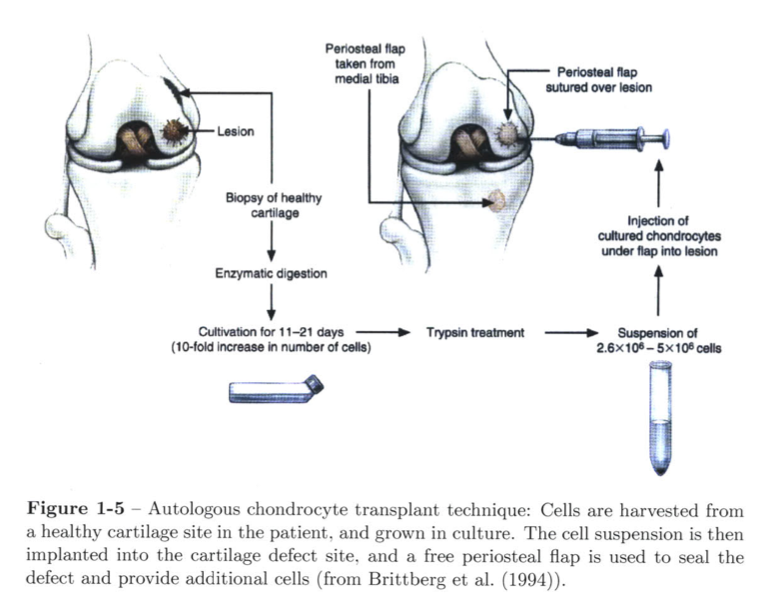
The first thing we notice is that the fact that these giants all had “big ears” means that there was an exaggerated, excessive amount of cartilage formation. Ears are made of cartilage how I don’t know at this time what type of cartilage the ears are made of. The protruding head reminds us of many pituitary giants with protruding heads. From the picture above on Siah Khan we see that his condition is very severe.
 Note: A good example of just how enlarged Proteus Syndrome can make human body parts, but especially the limbs (aka appendicular skeleton areas) is the case of Mandy Sellars which is shown on the left. And NO, that picture is NOT photoshopped. Her condition is real and can show just how severe and detrimental proteus syndrome can be to the human body.
Note: A good example of just how enlarged Proteus Syndrome can make human body parts, but especially the limbs (aka appendicular skeleton areas) is the case of Mandy Sellars which is shown on the left. And NO, that picture is NOT photoshopped. Her condition is real and can show just how severe and detrimental proteus syndrome can be to the human body.
From Mandy Sellars website on the Proteus Syndrome we would find the symptoms on the condition…
What is Proteus Syndrome?
Proteus Syndrome is a condition which involves atypical growth of the bones, skin, head and a variety of other symptoms.
The name comes from the greek God Proteus who used to change his shape or form.
it is very rare, variable and progressive, affecting more males than females and the cause of is unknown.
The syndrome became more widely known when Joseph Merrick (the patient depicted in the play and movie “The Elephant Man”) had severe Proteus syndrome rather than Neurofibromatosis as had been previously suggested.
What are the signs?
1. Overgrowth, asymmetry (none symmetry) and gigantism of the limbs.
2. Increased size of an organ, or the body, or bones aka Hypertrophy
However again I would go off on a side tangent on my research and need to come back to the original forum thread. The names of a Robert Melvin would be mentioned who is well known for his puffy face who was called The Man With Two Faces. He suffering from Neurofibromatosis. (source)
Roger would make more informative comments with…
“I dont know how symmetric is the overgrowth that McGrory and the others show on his heads, but I agree that they have very specific features like those protruding temporal lines in both sides of their head, sloped foreheads, etc…”
It would seem that the forum members would find that Siah Khan had a syndrome named after him called “Ghorban-Sheikholeslami-Shafeghati Syndrome“. The issue the posters note is that of the four giants we are looking at, 3 of them are dead. Only the guy the forum labeled “tallest filipino” is apparently still alive, and if we can him to agree for a genetic analysis we might be able to diagnose from a genetic perspective what is causing this condition.
The ending is what really brings the discussion to something reasonable in science validation. Apparently a study and paper was done on the curious case of Zech Devits. The paper is entitled “A provisionally unique syndrome of macrosomia, bone overgrowth, macrocephaly, and tall stature” by Ab Sadeghi-Nejad, and Lawrence I. Karlin. Article first published online: 18 MAR 2005
The abstract is below (Note: A full text of the paper is not available off of say PubMed but is available on the forum HERE …
Abstract
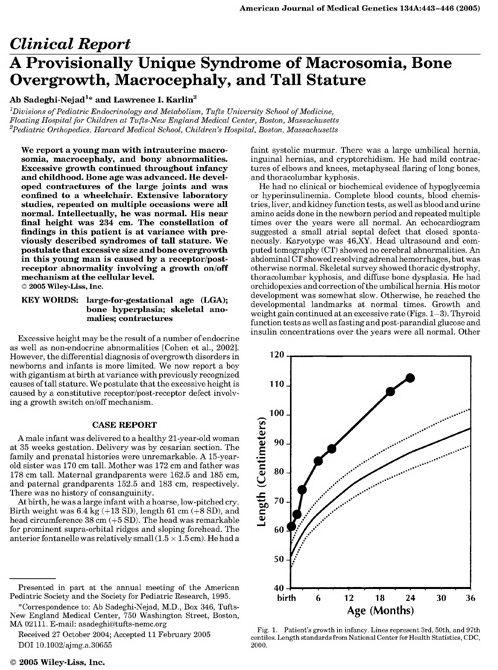
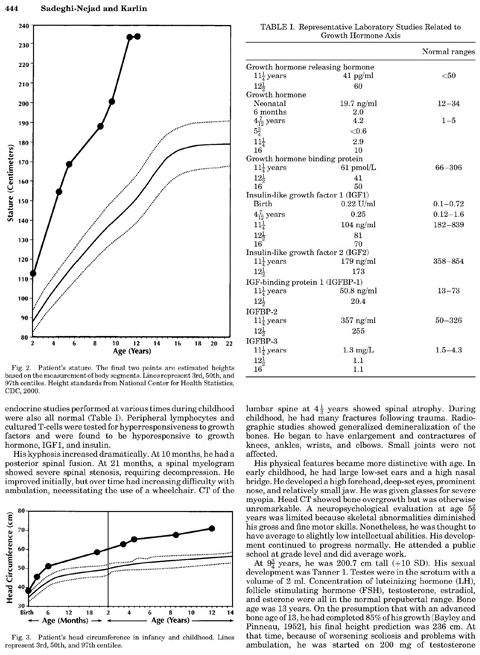
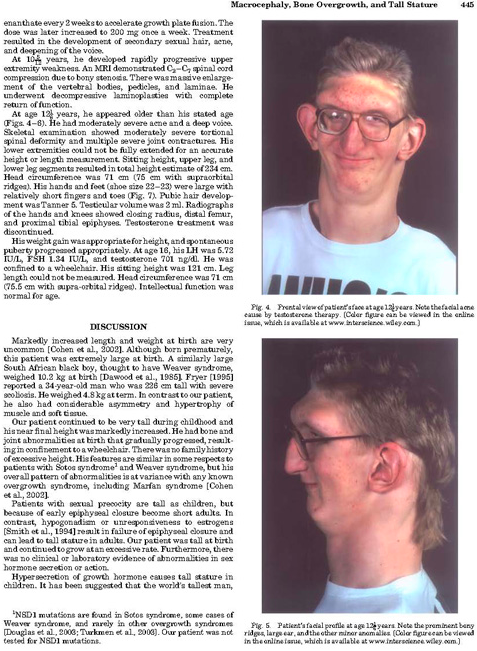
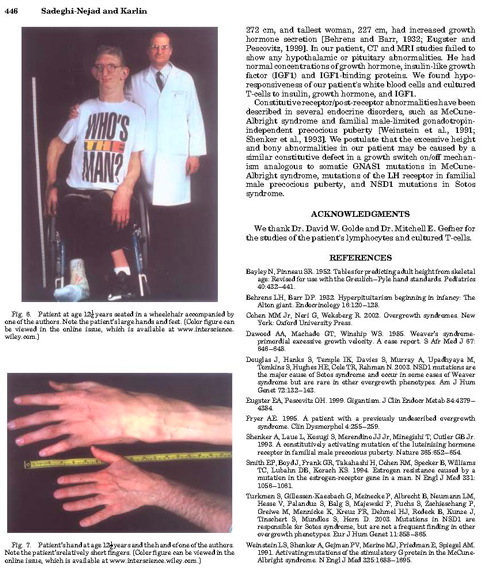
We report a young man with intrauterine macrosomia, macrocephaly, and bony abnormalities. Excessive growth continued throughout infancy and childhood. Bone age was advanced. He developed contractures of the large joints and was confined to a wheelchair. Extensive laboratory studies, repeated on multiple occasions were all normal. Intellectually, he was normal. His near final height was 234 cm. The constellation of findings in this patient is at variance with previously described syndromes of tall stature. We postulate that excessive size and bone overgrowth in this young man is caused by a receptor/post-receptor abnormality involving a growth on/off mechanism at the cellular level. © 2005 Wiley-Liss, Inc.
Conclusion: This post is getting way too long so I will cut it off here and continue this new discovery in a next post. What is amazing to note is that these men all seemed to have suffered from some genetic disorder to cause them to develop extreme height. Zech was found to have a height of 234 cm which is over 7′ 8″ even though he would eventually be confined to a wheelchair, just like Matt Mcgrory. The analysis on a more scientific level will be done in the subsequent posts.