Recently I got a message or comment to the website where someone would link to a study that Tyler from HeightQuest.com had written about in the post “Reverse Ossification”
The study or article was entitled “Growth Plate Reappearance after Closure in Ankle Radiography for Trauma“
Article abstract:
Bone growth plates or physis are present at the end of long bones and are responsible for longitudinal growth. These plates consist of 4 layers and are lucent in radiography as a line perpendicular to the longitudinal axis, Because of cartilage layer x-ray absorption is less than calcified bone. Gradually increases with age and bone maturity these line will be narrower and as longitudinal bone growth stops, the line disappears. This phenomenon occurs at different ages in different bones of the skeleton but with complete maturity at the age of 19, all growth plates are closed and sclerosed. Re-appearing after closing is uncommon. We introduce two young patients in this study due to trauma have been treated for an ankle cast and the growth plates of tibia and fibula in their control X-ray was re-appeared. Subchondrel Bone Resorbtion is a known phenomenon that will occur after 6 to 8 weeks immobility in any bone. The lucent line caused by imbalance in osteoblast and osteoclast activity and bone absorption. Re-appearing of growth plates can be caused by reversed ossification and bone absorption.
Analysis
Months ago Tyler had brought the article to my attention when he asked for my help in finding some way to translate the article written in Persian/Farsi since the article was written by medical researchers based in Iran. I tried using Google Translate and Yahoo’s Babel Fish technology without success.
After getting some extra time to looking back at the study and really think over what is really going on, I wanted to make some observations about what is going on. The first thing I see is that the doctors say that “Re-appearing after closing is uncommon”
The way they word the phrase makes a person who is really intent on finding a way to reverse the ossification think that maybe the reappearance of growth plates happen a lot more often then say “NEVER”.
Are these researchers saying that they have seen growth plate reappearance before in other cases? Because I have not in any studies, medical textbooks, or journals.
Here is what I guess is really going on. The cartilage is indeed there. The X-rays they see show that the absorption rate is lower. If we look at how X-rays turn out, we remember that the calcified bones will absorb more so the color on the X-rays is much lighter, or transparent. The less absorption on X-rays turn out darker and less transparent.
 What you see in the article which Tyler copied to the Post is a series of X-rays but I would say even after looking at long bone X-rays before that I can’t really see what the growth plate is supposed to have regenerated.
What you see in the article which Tyler copied to the Post is a series of X-rays but I would say even after looking at long bone X-rays before that I can’t really see what the growth plate is supposed to have regenerated.
The picture to the right is the only X-rays where I am noticing any type of mark or fracture in the bones. If we look at the way the dark line is on the bone, I would say that the line is very straight, and not curved and crooked like how the cartilage appears in young pig ankles, which I showed in one of the website’s YouTube video HERE
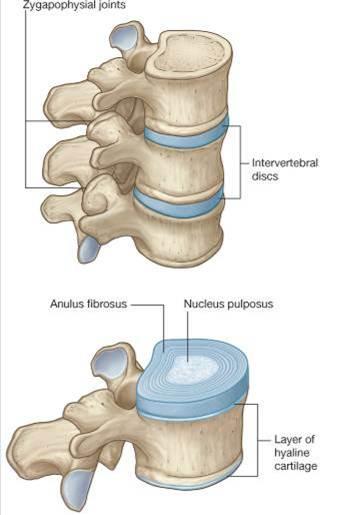
At this point, I would say that the darker shade of line on the tibia area is not the hyaline growth plate cartilage coming back but something else.
That something else I am proposing is actually fibrocartilage. Fibrocartilage is what would be formed if you managed to puncture or lacerate the bone deep enough to get below the subchondrel layer of the cortical bone.
When I was doing research on the subject of microfracture surgery I wrote a post about the possibility of using microfracture surgery to grow taller entitled “Increase Height And Grow Taller Using Microfracture Surgery, Part I”
From the Wikipedia article….
Through use of an awl, the surgeon creates tiny fractures in the subchondral bone plate.[9] Blood and bone marrow (which contains stem cells) seep out of the fractures, creating a blood clot that releases cartilage-building cells
Analysis
The principle of microfracture surgery results in the fact that the cells in the bone marrow will seep out and the progenitor adult stem cells will first differentiate into the chondrogenic lineage, at least at first.
All the physicians are in agreement that when the surgeon uses the awl to drill a hole into articular cartilage, the cartilage that is formed is fibrocartilage, not hyaline cartilage. In the procedure section on how microfracture surgery is done, the awl is a drill tool that goes pass the hard cortical bone layer and reaches to the spongy, more porous cancellous bone area where the marrow and adult progenitor cells are.
And this is what I think is really showing up in the X-rays of this document that Tyler and the other person found. That straight dark line that slices horizontally across the X-ray I am saying is more likely a bone fracture that is mostly likely filled with progenitor cells which wil turn it into fibrocartilage, not the hyaline type of cartilage the Iranian researchers claim them to be.
I wrote about a proposed idea on how we could theoretically use the fibrocartilage that is formed to increase our height at “A Proposed Height Increase Method Using Microfracture Surgery Techniques With Fibrocartilage Formation”
Perhaps there might be a possibility to combine the propose method from the post above with trauma injury type os incidents which lead to X-rays showing fibrocartilage formation. I said in the recent post that to do reverse ossification properly, we would have to have at least two major stages that not only happen at the same time, but also happen sequentially. they are…
1. One step would be to somehow remove the hard inorganic, nonliving tissue between the bone cells (osteocytes) and lacunae in the extracellular matrix of the bones.
2. The second step would be to be able to cause only chondrogenesis (to create cartilage) to occur in the area which lost the inorganic nonliving tissue.
Remember that ossification is where either the chondrocytes turns into osteocytes and osteoblasts or they die leaving the spaces for the osteocytes to take up later in development.
This is like how life goes. You can either turn into something else through evolution or a transformation or you die out to be replaced by something else. If you want that process to go in reverse, you would either have to figure out how to do transdiferrentiation, which the immortal hydra had figured out how to do, or you have to figure out how to reverse in the aging process, which the immortal hydra also figured out.
Since we are not talking about the entire body as an organism, but also a section of our body to regenerate back the cartilage we lost from the natural growth process, it would be much easier to first remove the dead, non-organic, hard calcium miineral deposits first. After the deposits are removed, then you replace over the now empty space with cartilage forming chondrocytes with some type of injection or growth factor mixture.
I would conclude with two things.
- The X-rays is not showing growth plate hyaline cartilage re-appearance, but actually some type of fracture that was made by the injury. The bone is cracked and maybe some other body tissue has gotten into the bone cracked region.
- If the X-rays is not a fracture, but actually cartilage, then it is not the hyaline cartilage we are looking for, but actually fibrocartilage that has seeped out of the cavity and the trabecular bone from the inside.
Let’s look at what is stated in the beginning of the young kids who are getting their X-rays looked at.