This Ph.D Thesis & Dissertation was interesting because it seems to talk about the mechanical properties of the human femoral bone, which has been something that I and some other height increase researchers have been searching for a long.
Ph. D Thesis: The Distribution and Importance of Cortical Thickness in Femoral Neck and Femoral Shaft and Hip Fracture and Lower Limb Fracture – Author: Fjóla Jóhannesdóttir
I wanted to list a few parts of the thesis which will help us gain a better understanding on the physiology of the adult human femoral bone
Bone Biology, Introduction 2.1 – Bone require mechanical stress in order to grow and strengthen therefore physical activity is important to develop and maintain bone strength.
2.2 Structure of Bone – The composition of bone is more complex than most engineering composites as there is no level of organization at which one can truly be said to be looking at bone as such.
2.2.1 Composition of bone – Bone is composed of 65% (by weight) mineral (inorganic phase) and 35 % organic matrix (consist of 90% collagen and 10% of various noncollagenous proteins), cells and water (Jee 2001).
- Composition of Bone Continued – The bone mineral is in the form of small crystal in the shape of needles, plate, and rods located within and between collagen fibers. The mineral is largely an impure form of naturally occurring calcium phosphate, most often referred to as hydroxyapatite Ca10(PO4)6(OH)2
- Calcium compounds provide stiffness and strength but collagens provide ductility and toughness (Currey 2003).
- During growth, the amount of organic matrix per unit volume remains relatively constant, while the amount of water decreases and the proportion of bone mineral increases. The reduction of water content results in a stiffer bone in adults than in children.
2.2.2 Bone cells – The major cellular elements of bone include osteoclasts, osteoblasts, osteocytes and bonelining cells.
- Osteocytes – are the principal cell type in mature bone and derived from osteoblasts. They are embedded into bone matrix, residing in lacunae and communicate with neighbouring osteocytes and with osteoblasts and bone lining cells by means of processes that are housed in little channels (canaliculi)….Aging, loss of estrogen, loading, and chronic glucocorticoid administration is known to increase osteocyte death (Noble and Reeve 2000).
- Osteoclasts – …Actively resorbing osteoclasts are usually found in cavities on bone surfaces, called resorption cavities. When osteoclasts have done their job they disappear and presumably die. The osteoclasts possesses receptors for calcitonin and responds to parathyroid hormones, 1,25(OH)2, vitamin D3 and calcitonin. Bisphosphonates, calcitonin and estrogen are commonly used to inhibit resorption and are believed to act by inhibiting the formation and activity of osteoclasts and promoting osteoclast death
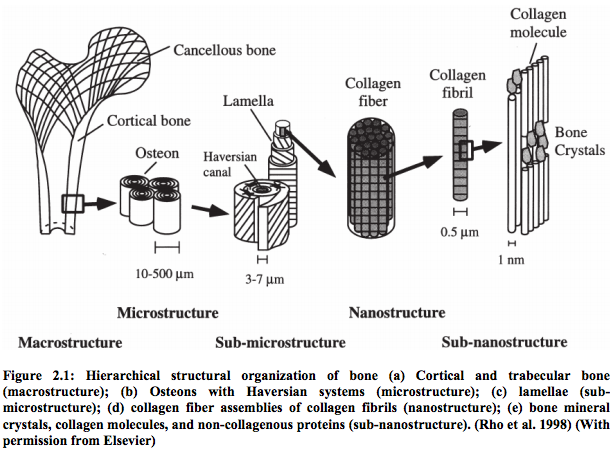
2.2.3 – Hierarchical Levels of Bone (from lowest to highest)
Note: Human bones have an irregular arrangement and orientation of the components, making the material of bone heterogeneous and anisotropic.
- Sub-nanostructure – a molecular structure of constituent elements, such as mineral, collagen and non-collagenous organic proteins
- Nanostructure – a composite of mineralized collagen fibrils
- Sub-microstructure – the fibrils are arranged in two forms, woven bone and lamellar bone.
Woven Bone
- is characterized by irregular organization of collagen fibers
- is mechanically weak
- usually laid down very quickly
- found in situations of rapid growth in children and during initial stages of bone fracture healing
Lamellar bone
- is more precisely arranged.
- The collagen fibrils and their associated mineral are stacked in thin sheets called lamellae (3-7µm wide) that contain unidirectional fibrils in alternate angles between layers.
- Lamellar bone is most common
- can take various forms at next level (microstructure).
- Primary lamellar bone is new bone that consists of large concentric rings of lamellae
- Macrostructure – there are two types of bone, cortical bone and trabecular bone (aka cancellous bone)
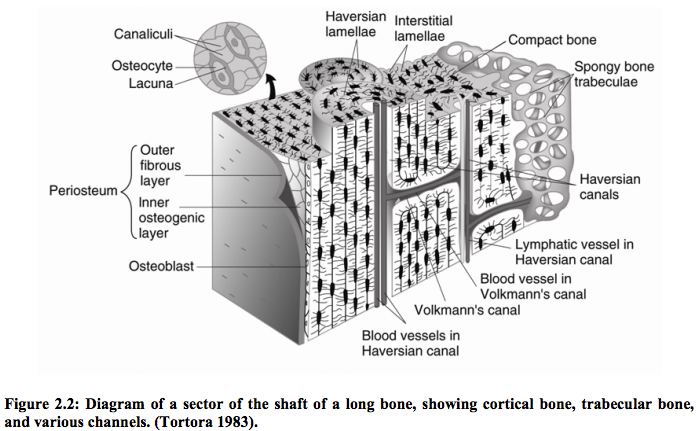
1. Cortical bone – is made of Haversian systems (aka osteons)
The most common type of cortical bone in adult human is called osteonal (aka Haversian bone)
Haversian bone
- contains blood vessel capillaries
- nerves
- a variety of bone cells.
The substructure of concentric lamellae, including the Haversian canal, is termed an osteon. It looks like a cylinder.
Other channels
- Volkmanns’s canals – run perpendicular to the Haversian canals providing radial paths for blood vessels.
2. Trabecular bone
- a highly porous cellular solid
- the lamellae are arranged in an interconnecting framework of trabeculae in a form a series of rods and plates
The picture below is taken from Page 5 if the Ph. D Thesis, which seems to have been taken from Elsevier
2.2.4 – Cortical & Trabecular Bone
Trabecular Bone
- is much more porous with 50-90% porosity and is usually found at the ends of long bones
- in cuboidal bones and flat bones like the pelvis
- overall matrix forms an open network of trabeculae (interconnecting rods or plates of bone) and spaces are filled with marrow.
- are oriented along stress lines and the surface covered with endosteum.
- have no blood vessels and the canaliculi are opening on surface and nutrition are transmitted through them.
Cortical Bone
- is solid, with only spaces in it being for osteocytes, canaliculi, blood vessels and erosion cavities.
- It is much more dense and stronger than trabecular bone with 5-10% porosity.
- Approximately 80% of the skeletal mass in the adult human skeleton is cortical bone.
- It is primarily found in the shaft of long bones and forms the out shell around trabecular bone at
- the end of joints and the vertebrae
2.3 – Bone Modelling & Remodelling
Ossification and skeletal growth require two essential processes, 1. bone modelling and
2. bone remodelling.
Bone Modelling
- consists of changes in bone shape and size to allow growth and adaptation to mechanical loading (Seeman 2009).
- Bone may be added to or removed from the periosteal and endosteal surfaces
Bone Remodelling
- old bone is removed under the signal delivered by damaged osteocytes and replaced with the same amount of bone in the same site of previous removal (Seeman 2009).
- is a balanced process – bone resorption and bone formation must equilibrate to prevent dysfunctions otherwise seen in bone diseases…
Frost´s mechanostat theory
- presents the relationship between bone formation, bone remodelling and the mechanical stimuli.
- describes a window of mechanical usage which is considered physiological and maintains the bone in homeostasis.
3.1 – Bone Strength Introduction
Bone has a number of mechanical properties and they can be described by…
- a load-deformation curve
- stress-strain curve
- Structural Behavior – the mechanical behaviour of a whole bone as a structure
- Material Behavior – the mechanical behaviour of the bone tissue
Load-deformation curve
- describes the relationship between load applied to a structure and deformation in response to the load and reflects the structural behaviour of the bone.
- the shape of this curve depends on both morphology and the material properties of the structure.
- The slope of the elastic region of the load-deformation curve represents the extrinsic stiffness of rigidity of the structure.
- Several other biomechanical properties can be derived including…1. ultimate load (failure load), 2. work to failure (area under the load-deformation curve), 3. ultimate deformation.
Stress-strain curve
- is analogous to the load-deformation curve but reflects the material behaviour of the bone that is independent of the geometry of the test specimen from which the properties were measured and it reflects the intrinsic properties of the material.
- The slope of the stress-strain curve within the elastic region is called the elastic or Young’s
- modulus that is a measure of the intrinsic stiffness of the material.
- The values of stress and strain at the ultimate point are ultimate stress and ultimate strain.
- The area under the stress-strain curve is a measure of the amount of energy needed to cause a fracture and is a measure of the toughness of the specimen.
- The elastic region and the plastic strain region of the stress-strain curve are separated by the yield point.
- Before the yield point, the bone is considered to be in the elastic region, and if unloaded, would return to its original shape with no residual deformation.
- In the post-yield region the stresses begin to cause permanent damage to bone structure.
- Post-yield strains represent permanent deformations of bone structure caused by slip at cement lines, trabecular microfracture, crack growth, or combinations of these
3.2 The Components that contribute to bone strength
Remember: The mechanical behaviour of a whole bone depends on…
- the morphology of the bone
- the intrinsic properties of the bone material itself.
Implication: Thus, properties at the cellular, matrix, microarchitectural and macroarchitectural levels may all impact bone mechanical properties
The factors that contribute to bone strength
- Bone morphology: Size, Shape (distribution of bone mass), Microarchitecture (trabecular architecture, cortical porosity/thickness)
- Bone tissue material properties: Density, degree of mineralization, extent of microdamage, collagen traits
- Bone turnover (Bone remodelling)
3.3 – Mechanical Properties Of Bone
- Bone is an anisotropic material – its mechanical properties are dependent upon direction of loading, leading in general to greater compressive strength than tensile strength.
- Bone exhibits viscoelastic behaviour – the elastic modulus and the strength of the bone are dependent on strain rate.
- Bone stiffness increases with increasing strain rate
- Ductility decreases with increasing strain rate.
- Material properties of bone, particularly stiffness and strength, are strongly dependent on the volume fraction and density.
- Cortical bone can withstand much greater load than trabecular bone but will not deform much before failure.
- Trabecular bone can deform significantly, but will fail at a much lower load.
The Cortical Bone – Mechanical Properties
- Cortical bone is both stronger and stiffer when loaded in the longitudinal direction
- compared with transverse plane because of the nature of the arrangement of the osteons
- Unlike the ultimate stresses, which are higher in compression, ultimate strains are higher in tension for longitudinal loading.
- In contrast to its longitudinal tensile behaviour, cortical bone is relatively brittle in tension for transverse loading and brittle in compression for all loading directions.
- Cortical bone is weakest when loaded transversely in tension and is also weak in shear.
- The mechanical properties of cortical bone are heavily dependent on porosity and degree of mineralization.
- More than 80% of the variation in the elastic modulus of cortical bone can be explained by a power-law relationship, matrix mineralization and porosity as explanatory variables.
- Cortical porosity can vary from less than 5% to 30% and is positively correlated with age.
- Thus, cortical bone properties for specific individuals depend on porosity.
The Trabecular Bone – Mechanical Properties
- elastic modulus can vary 100-fold even within the same metaphysis and with varying degree‘s of anisotropy
- mechanical properties should be accompanied by specifications of factors such as anatomic site, loading direction and age.
- the most important microstructural parameter for trabecular bone is its apparent density since the properties are often defined as a function of apparent density.
- Power-law relationships with bone density as the explanatory variable explain 60% to 90% of the variation in the modulus and strength of trabecular bone
- These power-law relationships indicate that small changes in apparent density can lead to dramatic changes in mechanical behaviour.
- it is important as stiffening the structure by holding together the shell, prevent buckling, support cortical bone in case of impact loads and distributes loads at extremities.
More Information About the Mechanical Properties of The Adult Human Femoral Bone
- while elastic modulus of cortical bone decreases modestly with aging, the strength and especially the toughness decrease more substantially
- In human cortical bone from the femoral mid-diaphysis, the tensile and compressive strengths decrease about 2% per decade
- While the toughness (energy to fracture) declines by 5-12% per decade, indicating that cortical bone becomes more brittle and less tough with increasing age
- These changes in the mechanical properties of cortical bone are mainly caused by the increase in porosity with age
- Other additional possible causes of the age-related deterioration of bone strength include changes in mineral crystal and collagen
- The elastic modulus and ultimate strength of trabecular bone decrease with age in both men and women as a consequence of markedly decrease in the apparent density
- The decreased strength of trabecular bone is also because of deterioration of trabecular architecture.
- Microdamage is another age-related change at both the cortical and trabecular tissue level which may contribute to bone strength
- As people grow older, the endocortical and intracortical remodelling increase resulting in that cortical bone becomes more porous and the cortex thinner
- As endosteal bone loss proceeds the periosteal apposition takes place that is an adaptation to maintain whole bone strength, increasing the cross-sectional area of bone to reduce the load/unit area (stress) on the bone and increase its resistance to bending and torsion
4.3 Whole bone strength of proximal end of femur in vivo
No notes were copied from the Ph. D for this section
Analysis
When I first started reading over this rather short Ph. D thesis I was expecting that the Ph. D. candidate would at least mention what the values and measurements for the mechanical properties of the human femur bone would be. It seems that after going over the thesis, I was unable to find any information on what I was really looking for. However, the thesis was a good read to review and refresh my memory on the elements and composition of bones in general.
The study was to show how changes in strength of the aging human proximal femoral neck would be. They were looking at how falls on the sides of elderly would result in fractures in the femoral neck area and hip fractures. They noticed that for women, nearly all the factors and parameters that determine bone strength decreased. Brittleness increased and area increased to compensate for increased bone porosity.
The researchers stated “We did not have an estimate of BMD or porosity in the femoral shaft cortex”