
Demineralized Bone Matrix is used as a scaffold to induce chondrogenesis and mineralized bone is an inhibition of interstitial growth which is how growth plates make you taller. Demineralized bone matrix binds fibronectin which may be necessary for chondroinduction. DBM also changes Wnt pathway signaling which may also affect chondroinduction. In fact, one paper suggests that bone growth on DBM occurs endochondral means which suggests that there is always a cartilage intermediate. Demineralized bone matrix also induced de novo endochondral ossification when implanted into muscle tissue.
If we could cause the demineralization of bone matrix just in certain spots that may enable the creation of growth plates in those particular areas.
Here’s what demineralized bone looks like:

“Bone mineral density (aBMD) is equivalent to bone mineral content (BMC) divided by area. We rechecked the significance of aBMD changes in aging by examining BMC and area separately. Subjects were 1167 community-dwelling Japanese men and women, aged 40-79 years. ABMDs of femoral neck and lumbar spine were assessed by DXA twice, at 6-year intervals. The change rates of BMC and area, as well as aBMD, were calculated and described separately by the age stratum and by sex. In the femoral neck region, aBMDs were significantly decreased in all age strata by an increase in area as well as BMC loss in the same pattern in both sexes. In the lumbar spine region, aBMDs decreased until the age of 60 in women, caused by the significant BMC decrease accompanying the small area change. Very differently in men, aBMDs increased after their 50s due to BMC increase, accompanied by an area increase. Separate analyses of BMC and area change revealed that the significance of aBMD changes in aging was very divergent among sites and between sexes. This may explain in part the dissociation of aBMD change and bone strength, suggesting that we should be more cautious when interpreting the meaning of aBMD change.”
So in men Bone Mineral Content increases with age. A lower bone density means more potential sites of demineralized bone in the bone. However, since BMC is only measured at certain sites it may be hard to extrapolate to the entire bone.
However, in some cases in aging bone area increases while BMC decreases which would be ideal for creating sites for de novo growth plate formation.
According to Sex-specific relationships between insulin resistance and bone mineral content in Korean adolescents., insulin resistance is linked to decreased bone mineral content. In one study, insulin resistance was linked to increased longitudinal bone growth. Maybe this is due to insulin resistance causing decreased BMC?
According to Cortical bone is more sensitive to alcohol dose effects than trabecular bone in the rat., alcohol decreases BMC but also decreases other bone parameters. Ideally, we’d only want a BMC decrease.
In some cases changes in bone architecture may decrease length:
“Bilateral ovariectomy was performed in female Sprague-Dawley rats under aseptic conditions and the rats were divided into five groups (n=10). Two different doses of methanolic extract of NR/CAL/06 (200 and 400 mg/kg, per oral (p.o.)) were evaluated for anti-osteoporotic activity and raloxifene (5.4 mg/kg, p.o.) was used as a reference standard. Treatment was given for 90 d.
The bilateral ovariectomy in rats resulted in decreased bone strength, bone mineral content and bone weight. The SEM images showed porous, perforated and disintegrated femur bone architecture and decreases in bone length and thickness in OVX rats. These changes were associated with elevated serum levels of calcium, phosphorus and ALP. Increases in body weight and adipose weight and a decrease in uterine weight were also observed and the changes were highly significant when compared with the sham-control group. Treatment with methanolic extract of NR/CAL/06 (200 and 400 mg/kg, p.o.) for 90 d dose-dependently restored the ovariectomy-induced alterations in bone weight, bone mineral content, bone strength, serum calcium, phosphorus and ALP, body weight and adipose weight nearly to normal levels. Furthermore, the SEM images of the femur bones of NR/CAL/06 (200 and 400 mg/kg, p.o.)-treated rats showed reduced pore formation and improved bone compactness compared with the OVX-control group.”
“The NR/CAL/06 is an herbal formulation consists of mixture of three different plant parts namely, Hibiscus rosasinensis (flowers), Cestrum diurnum (leaves){helps Vitamin D synthesis} and Glycyrrhiza glabra (whole plant){possess estrogen-like activity} in the ratio of 1∶1∶1. ”
The rats were 8 to 10 weeks old when the study began.
Femur length was actually slightly higher in OVX-control group than the sham control. NR/CAL/06 400mg group had longer femur length than both. The supplemented groups had a much larger variance of femur length than the sham control meaning that how much OVX or the supplements helps with height depends on the individual rat.
Effect of prior treatment with resveratrol on density and structure of rat long bones under tail-suspension.
“effects of resveratrol on bone mineral density (BMD), bone mineral content, and bone structure were examined in the femora and tibiae of tail-suspended and unsuspended rats using X-ray micro-computed tomography (micro-CT). Rats were treated with 400 mg/kg/day of resveratrol for 45 days and half of them were suspended during the last 2 weeks of treatment. Suspension caused a decrease in tibial and femoral BMD and deterioration of trabecular and cortical bone. Bone deterioration during suspension was paralleled by increased bone marrow area, which could be caused by an increase in stromal cells with osteoclastogenic potential or in adipocytes. Resveratrol had a preventive effect against bone loss induced by hindlimb immobilization. In particular, trabecular bone in the proximal tibial metaphysis was totally preserved in rats treated with resveratrol before tail-suspension.”
“[Resveratrol] increases epiphysial bone mineral density (BMD) and inhibits the decrease of femur calcium content in ovariectomized rats”<-interesting that this increasing in bone mineral density is in the epiphysis.
Tibia length in mm
Control
Nonsuspended: 41.58 ± 1.14
Suspended: 42.63 ± 0.68
Resveratrol
Nonsuspended: 40.90 ± 0.33
Suspended: 40.60 ± 0.57
Resveratrol decreased bone length and eliminated the bone length advantage from the suspended group. Note that the suspended group had longer bones than the non-suspended group. Also, remember that growth rate does not necessarily affect total growth. So this change in growth rate would not necessarily be reflected in adult height.
Cortical BMD was lower in the suspended group thus possibly suggesting an inverse relationship between BMD and height. The two resveratrol groups had the highest BMD.
Femur length
Control:
Nonsuspended: 37.73 ± 0.80
Suspended: 38.38 ± 1.06
Resveratrol
Nonsuspended: 38.75 ± 0.56
Suspended: 37.80 ± 0.32
In the femur the resveratrol nonsuspended femur growth was the highest and it was tied for having the highest bone density.
“In the tibial middiaphysis, measurement of marrow area showed an 1.3-fold increase after 2 weeks of tail-suspension compared to control animals. Resveratrol treatment prevented this increase. In the femoral middiaphysis, the increase in marrow area in suspended rats was more pronounced (1.5-fold compared to unsuspended rats) and could not be totally prevented by resveratrol pretreatment (resveratrol-treated suspended rats showed an 1.2-fold increase in marrow area compared to control rats).”
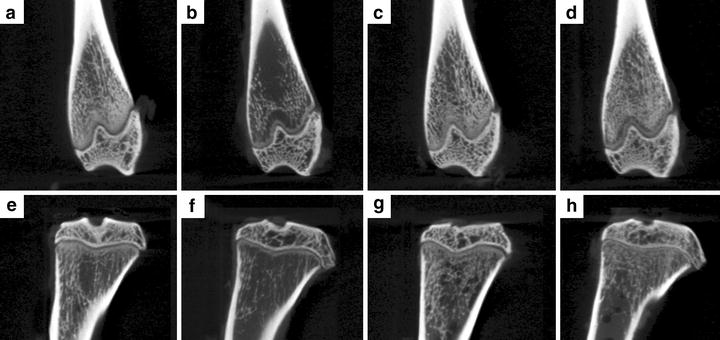
“Micro-computed tomography (micro-CT) slices showing femoral distal (a–d) and tibial proximal (e–h) metaphysis. Suspended rats (b, f) present less trabecular bone than control (a, e), resveratrol-treated (c, g), and suspended + resveratrol-treated rats (d, h)”
“There are mainly two sites that regulate bone structure and bone mass by responding to mechanical stress: one is the osteocytes, surrounded by bone tissue and the osteoblasts next to the osteocytes, and the other is bone marrow composed of mesenchymal and hematopoietic cells. Osteoblasts differentiate from mesenchymal cells and osteoclasts from hematopoietic cells”<-our goal with LSJL is to cause chondrogenic differentiation from mesenchymal stem cells.
According to [Relationship between bone mineral content and growth disorders in children with juvenile idiopathic arthritis]., growth inhibition was associated with lower bone mineral density.
Effects of Khaya grandifoliola on red blood cells and bone mineral content in rats.
“The therapeutic efficacy of a crude water extract of Khaya grandifoliola has been established in mice. This study was designed to assess the effect of the extract on the red blood cells and bone for 7 days, 3 weeks and a recovery period of 3 weeks. Daily administration of the extract showed no related adverse effects on the mortality rate, physical appearance or behaviour of the rats. A general pattern of significant increases in the red blood cell (RBC) count, PCV, haemoglobin and plasma iron content was shown by groups administered with extract after 7 and 21 days when compared with control rats. There was a general trend of reduction in the bone minerals determined (Ca, P, Mg and Cu) in the extract administered groups. Significant decreases were observed at the 500 mg/kg concentration. The bone potassium and iron content was significantly increased in rats administered with extract in a dose-dependent manner. There was an observed significant decrease in alkaline phosphatase (ALP) activity in the rats administered with the extract when compared with the control animals. During the recovery period, the haematological indices regressed to values which were still significantly higher than those of the control values. These results indicate that K. grandifoliola has a positive effect on erythropoeisis, but no significant effect on bone mineral contents at therapeutic doses. At extremely high doses and during prolonged administration, it may have an adverse effect on bone minerals.”
The red blood cell count of the 500mg/kg is 23% than the control group. 500 mg/kg also reduced phosphorus, calcium, zinc, and magnesium levels but not iron levels nor potassium levels(which were higher than control). Perhaps this could decrease the tensile strength of the bone making it more susceptible to stretching forces.
Khaya grandifoliola also decreased alkaline phosphate levels.
There haven’t been a lot of studies on khaya grandifoliola but if reducing bone mineral content does help in a height increase routine that involves stretching the bones than compounds derived from khaya grandifoliola will be extremely helpful.
The study also stated that “Most of us are the tallest at around 30-35 years old because of the peak bone mass at that time.”
However, BMC is useful when fighting against the forces of gravity in instances such as suspension then BMC content could be a detriment to the stretching of bones.