Summary:
* LSJL increased right finger to be longer than the left. Need X-ray to see if there are growth plates. Easiest way to do this?
* LSJL increased left thumb over right thumb. Thus LSJL can be reproduced.
* There are indications that LSJL is effective at increasing leg height.
* Clamping at the knee may be more effective than clamping at the ankle due to structural differences.
As you know, I’ve proven that due to LSJL my right index finger is now longer than my left. The issue is that people are “So what?” They don’t understand that the finger is made up of long bones(albeit with slightly different properties than the leg bones) and if you can induce length increase there it follows that you can increase bone length in the legs as well.
Originally, I ruled out getting an x-ray because people wouldn’t care about an increase in finger length but if I have successfully recreated a growth plate then that would successfully prove LSJL for the masses. The problem is actually getting an x-ray of ideally both hands without having to get a doctors appointment first (and paying out of pocket for that). I just want to go in, get an X-ray and then pick it up. I can afford it for the $200ish I’ve seen especially since it’ll prove LSJL. There’s a risk that there won’t be a growth plate but I am absolutely positive that my finger has grown longer by some mechanism and that it’s not due to bone thickening. It is possible that it grew by some mechanism relating to articular cartilage endochondral ossification but people with osteoarthritis have endochondral ossification and I have not found any reports of bone lengthening.
So how can I get a hand X-ray with as little medical red tape as possible? I want to walk in, get the x-ray, pay, and pick it up.
I’ve also been loading my left thumb and there’s a small but significant and noticeable difference between my left and right thumb. I’m working on finding the best way to photograph it. It does establish that the finger lengthening is not a fluke and is reproducible.
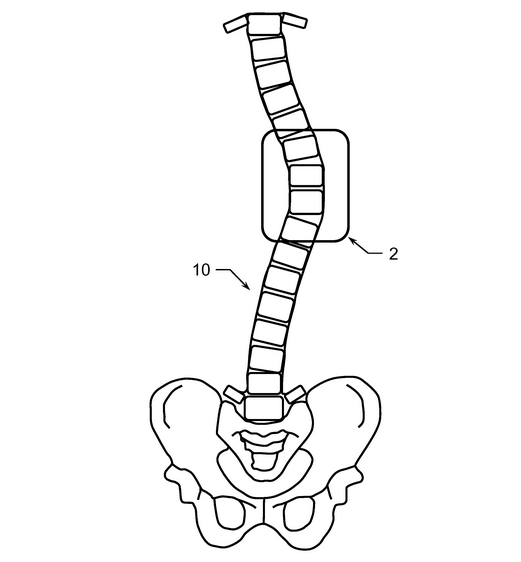
Another good sign is my legs. My epiphysis has been changing in shape to become more hammerhead in appearance like my fingers dead. Even if LSJL induces such “deformities” it would certainly be worth it to some people to grow taller.
And it seems as though my left leg is now longer than my right. The renewed growth can be explained by the following: I used to load my leg with a C-class clamp but now am using an Irwin Quick Grip to reduce slippage. Now I am focusing much more on intensity of clamping but with shorter duration
(Note: Since I cannot yet specify an ideal intensity I cannot guarantee against injury!).
Now I always used the Irwin Quick Grip on my ankle but didn’t really get good results there and haven’t seen a lot ankle changes despite clamping harder. I think the reason for this could be that the knee is different structurally than the ankle and it makes LSJL more effective on that area.
So the reason why this routine could lengthen my left leg more than my right is that I load my left leg first as it is my weaker leg. If I can get up to say a count of 130 on clamping my left leg(starting over at 0 if the clamp slips) then I clamp to 130 on my right leg. So my left leg is guaranteed to get maximal clampage whereas the right leg is not.
Now there are other explanations as to why I feel my left leg has grown longer than my right:
1) Placebo effect. I want my left leg to be longer to prove LSJL. Although when I extend my legs my left leg is longer than my right and if I stand on my left leg I’m taller then if I stand on my right leg.
2) Hip Rotation. Which would explain the symptoms of the left leg extending longer without any actual lengthening. But what would be the stimulus?
3) My left leg has always been longer than my left. I think I would’ve noticed it before.
So this effect isn’t perfect proof of LSJL but I think with the devolpment of more hammerhead-esque bones it is a good sign of LSJL’s effectiveness in increasing leg height.
——————–
Michael: One could go to Urgent Care, which is a type of walk-in facility which would let one get their bodies X-rayed. You’d still have to pay the costs though, but it would be faster. When I was looking at how deer antlers grow, I noted that the antlers where able to grow in length only because there was no physical constraint against the upper horn part from getting longer. Human legs have that constraint since we have to constantly be putting loadings on the feet from walking. if we could put our bodies into some bed for months on end while clamping, maybe there would be much bigger results. The effects on fingers, which are just jutted out and not being pushed down consistently on a flat surface would see much more noticeable effects.