
The below paper has some insight into supplemental and genetic factors that influence height that I have not seen before.
Nutrition, Other Environmental Influences, and Genetics in the Determination of Human Stature.
“It has been proposed that human linear growth goes through phases of saltation and stasis, with short bursts of rapid growth (up to 1.65 cm within a single day) between long periods (7–62 days) of no growth at all. However, saltatory growth was not observed in human studies by other groups or in other mammals using highly precise radiological measurements. From the perspective of growth plate biology, the continuous nature of chondrocyte recruitment, proliferation, and hypertrophy is inconsistent with long periods of inactivity punctuated by acutely robust proliferation and hypertrophy. Therefore, the hypothesized model of human saltatory growth remains somewhat controversial.”<-If it is possible to grow 1.65 cm in a single day then that means that there must be a way to get around soft tissue limitations in limb lengthening surgery.
“senescence is dependent on growth itself rather than on chronological age. To put it another way, chondrocytes in the growth plate might have a finite amount of growth potential, which is gradually exhausted, leading to the decline in growth rate and associated senescent changes.”<-but that does not mean that we can not alter growth plate senescence.
“On the basis of the assumption that growth itself drives growth plate senescence, growth-suppressing conditions such as nutritional deprivation or inflammation may preserve growth potential and delay senescence”<-there may be ways to trick the growth plate to think that it needs to delay senescence even while it is still growing normally. Possible mechanisms to do this may be via SIRT1.
“Childhood stunting in the first 2 years of age is associated with reduced stature in adulthood, suggesting some permanent loss of growth potential to some degree, despite catch-up growth.”
“Endocrine factors controlling embryonic and somatotrophic fetal growth are of placental and fetal origins and include insulin-like growth factors I and II (IGF-I and IGF-II), growth hormone 2 (GH-2), and human placental lactogen (hPL). In addition, the thyroid hormones thyroxine (T4) and triiodothyronine (T3) play a central role and impact tissue accretion and differentiation as well as having an indirect role in controlling the effectiveness of other hormones including IGFs. GH-2 or placental growth hormone directly affects placental development but is also correlated with IGF-I. While IGF-II is involved in early pregnancy, in late gestation, IGF-I, synthesized in the fetal liver in response to insulin levels determined by glucose availability, controls fetal growth. hPL is secreted by the placenta and is a somatogenic hormone. Glucocorticoids can impact fetal growth, although the presence of a barrier enzyme (11-β hydroxysteroid type 2) converts maternal cortisol, which may inhibit fetal growth, to cortisone”<-what would happen if things like GH-2 and IGF-2 were upregulated in adults?
“GH excess caused by pituitary adenomas leads to elevated IGF-I and gigantism, while GH deficiency in children leads to decreased IGF-I and stunted growth. Like many other hormonal axes, IGF-I provides negative feedback to limit GH secretion in the pituitary. Therefore, children with GH receptor mutations develop a condition called GH insensitivity, where target tissues produce a muted response to circulating GH, leading to increased GH but decreased IGF-I in the circulation and poor linear growth.”<-the GH receptor may be why gigantism is so rare and HGH does not always increase height drastically. The GH receptor may adapt to excess GH.
“Because FGF21 can signal via FGFR3, it is expected to suppress bone growth in rodents via activation of FGF signaling. What is unexpected, however, is that FGF21 can also suppress bone growth in part by inducing GH resistance both in the liver and at the growth plate. A transgenic mouse model with overexpression of FGF21 showed decreased GH-induced STAT5 (signal transducer and activator of transcription 5) signaling and, consequently, diminished hepatic and local expression of IGF-I”<-reducing FGF21 levels may be a way to increase height pre skeletal maturity.
“In both humans and mice, prolonged fasting increases circulating FGF21″<-This would suggest that fasting would reduce height. It may be possible to trick the body if you block FGF21 and fast, you may boost SIRT1 levels or some other mechanism that makes the body preserve catch up growth. So you may grow normally during fasting and then get the catchup period post fasting. You could also potentially block FGFR3 via some mechanism.
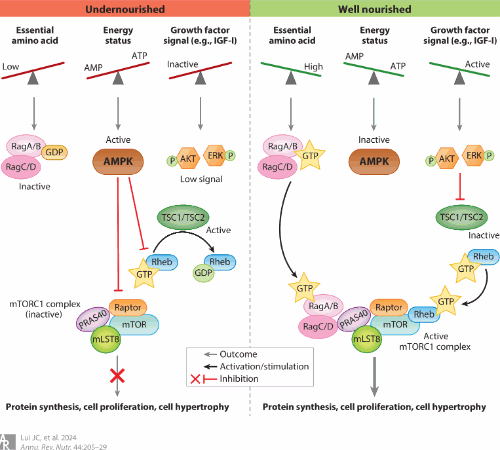
“nutrient deprivation may result in decreased local IGF-I signaling at the growth plate (due to GH resistance), followed by a reduction of AKT phosphorylation and decreased recruitment of the resting zone stem cell pool into the proliferative columns. Evidently, administration of exogenous IGF-I in the system was able to restore both AKT phosphorylation and recruitment of resting chondrocytes”
“Androgen itself may have an estrogen-independent effect on stimulating bone growth, because administration of a nonaromatizable androgen in boys has been shown to accelerate linear growth. Unlike that of estrogen, this effect does not appear to be driven by an increase in the GH–IGF-I axis, but rather by a direct, local effect on chondrocyte proliferation”
“[The] effect of estrogen on bone growth is the acceleration of skeletal maturation and induction of growth plate closure. In precocious puberty, premature estrogen exposure leads to advanced bone age, premature epiphyseal fusion, and decreased adult height. Conversely, in hypogonadism, the lack of estrogen leads to delayed fusion and tall stature. Much of this effect of estrogen on skeletal maturation is mediated locally at the growth plate, by accelerating the depletion of stem cells in the resting zone”<-the reduction of estrogen to increase height pre-skeletal maturity has been studied.
“leptin has a direct effect on growth plate chondrocytes that negatively impacts catch-up growth. Refeeding after undernutrition increased leptin levels, which stimulated local aromatase activity at the growth plate and in turn accelerated estrogen-driven skeletal maturation, limiting the amount of catch-up growth. These findings provided important mechanistic insights into why undernutrition often leads to incomplete catch-up growth and permanent growth deficit.”<-So leptin may increase growth rate but result in lower final height due to enhancing estrogens negative effects,
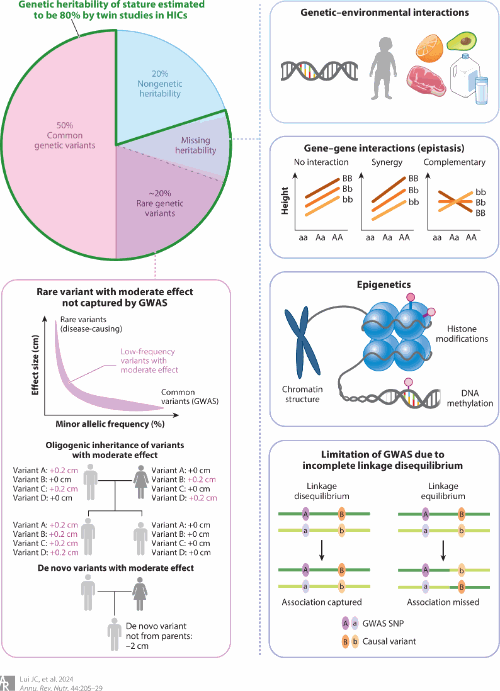
The image above suggests that we can alter genetics somewhat via epigenetics.
“Individual nutrients have been linked to growth and described as growth promoting, such as zinc, magnesium, phosphorus, and essential amino acids. Iron deficiency, common among children and a primary cause of anemia, will result in poor growth and development, and during pregnancy it causes fetal growth restriction due to hypoxia and increased maternal stress”<-We need to know how much of these nutrients are optimal and where more would have no additional beneficial effect.
“The importance of animal source protein and essential amino acids in promoting linear growth in children”
“gut microbiota dysbiosis leads to reduced plasma amino acids”<-this may be one of the ways in which the gut microbiome influences height.
“environment-driven changes in the gut microbiota can similarly affect linear growth via this pathway, animal research suggests that microbial metabolites may also directly stimulate IGF1 gene expression”