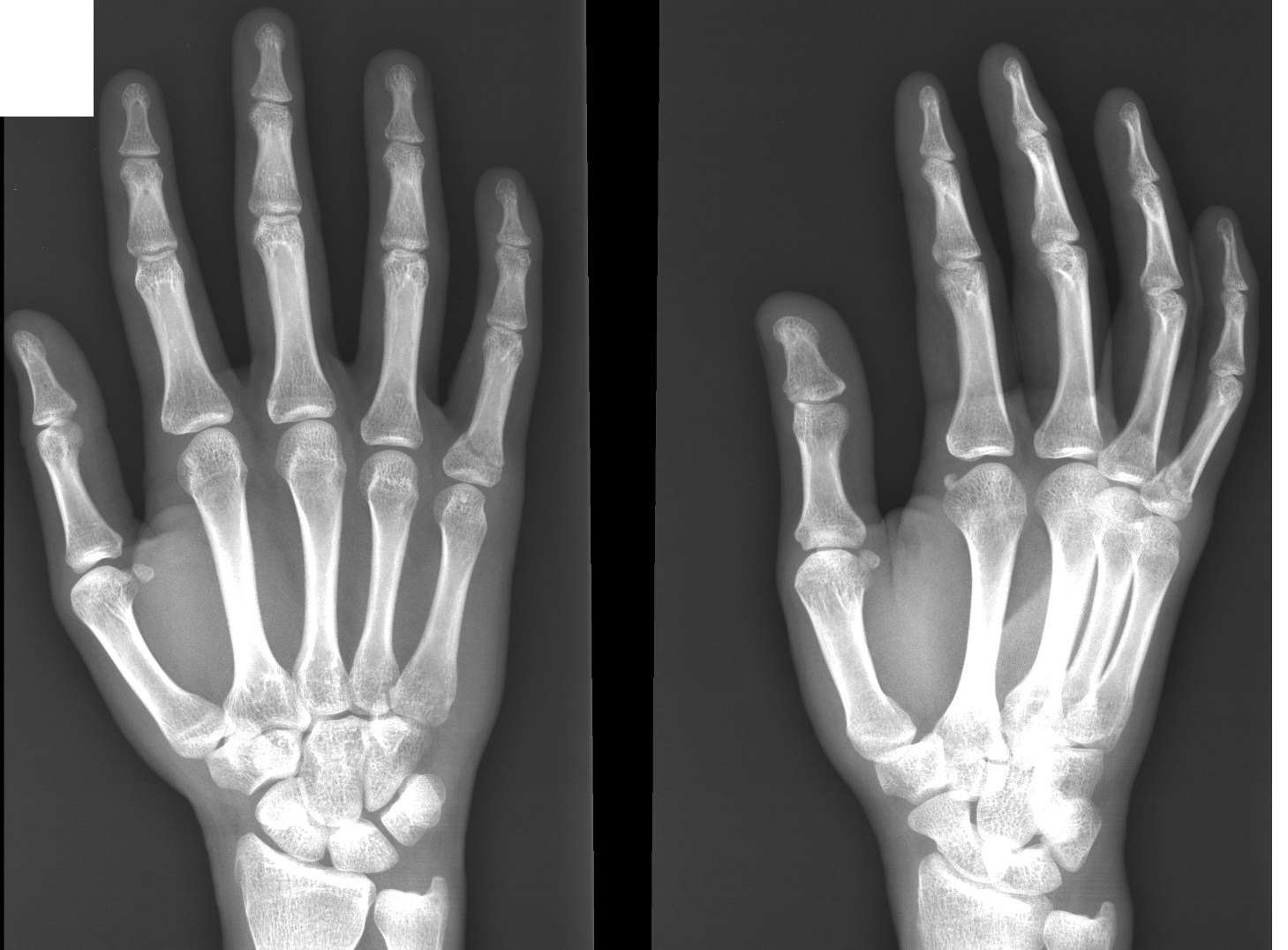
I’ve been working hard on trying to increase my hand and feet size via clamping and I’ve had some moderate measurable success and I’m working to get more.
The reason I chose the hands and feet was because I didn’t want to be limited by clamping strength in terms of getting results. I’ve hard to order clamps that aren’t available in hardware stores and I may have to get even stronger clamps.
But one things I didn’t consider was the shape of the bones and not just the size(hands and feet bones are smaller).
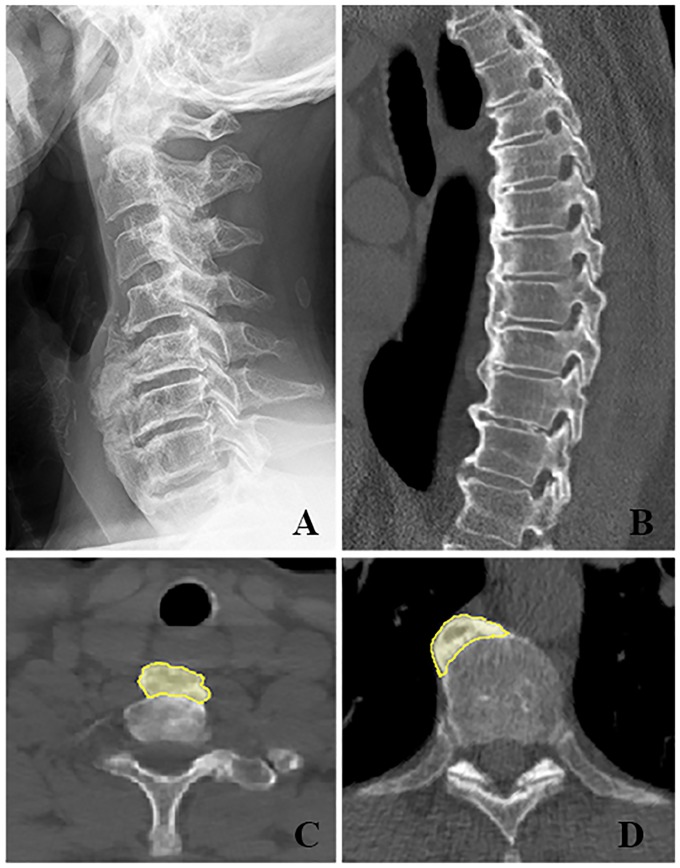
The curved nature of the ribs means that LSJL is going to be more effective think of water in a curved pipe rather than a straight one.
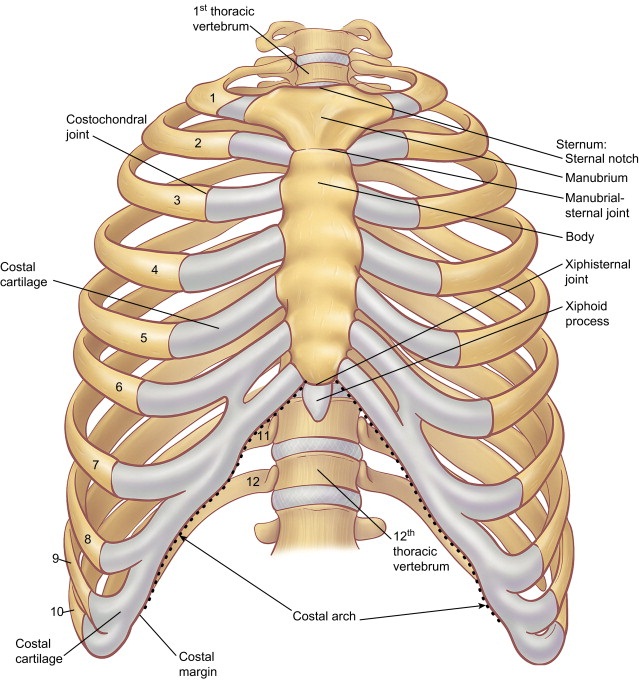
The fluid inside the bone is going to be bouncing around all the curvatures of the rib rather than just flowing down a straight line. And take a look at how much more cartilage there is in the ribs than there is normally that likely means that the rib bones will behave differently from long bones.
And there is already LSJL going on in the ribs, it’s called scoliosis bracing. However, it differ from LSJL in that it’s not on the epiphysis(the weakest part of the bone) and that the load is static(although you are moving around in the brace).
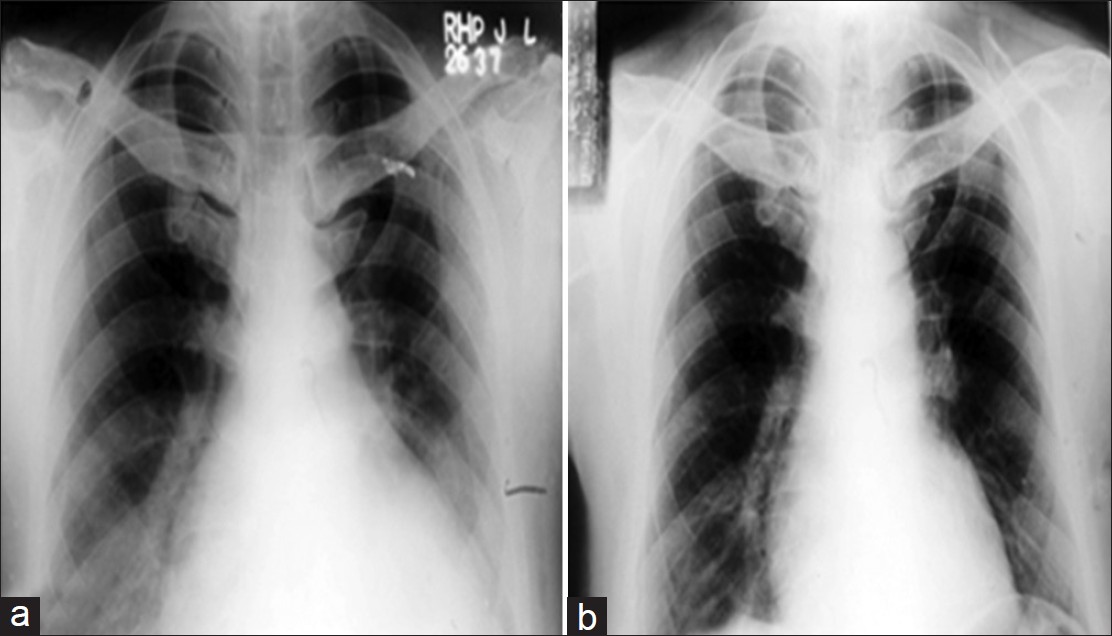
Just by breathing you’re doing LSJL on the rib cage by all the expansion pressing against the ribs.
There’s also been reports of people getting larger ribs via pullovers but that is not LSJL.
Papers like this one report growth in the rib cage due to age, Quantification of age-related shape change of the human rib cage through geometric morphometrics, I couldn’t get the full study but the study established correlation between thorax(basically rib cavity size, the larger your ribs the larger the rib cavity) and age, weight, and height with weight being the largest correlation. And weight can perform lateral loading on the epiphysis, it’s just that due to curved nature of the rib bones it needs a lot less load than other areas and people store a lot of weight in their torso.
And another region of interest is the jaw which has a lot of curves too and a lot of people are interested in the jaw due to it’s importance in sexual dimorphism and it’s perceived impact in male dominance. Thank of Michael Cera, Zach Braff, and James Ellworth in terms of jaws.
I’m already doing LSJL on the jaw but I’m going to be working harder at it. Then I’m going to figure out how to do a routine for the ribs.
I’ll see if I can find more evidence of rib growth over time(you can help) and post about it definitively at the next LSJL update.