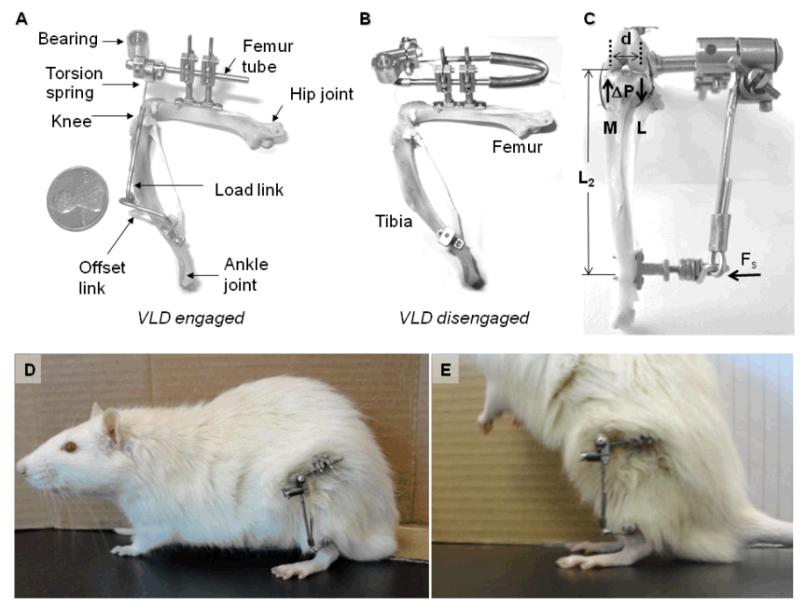
“This study describes the first application of a varus loading device (VLD) to the rat hind limb to study the role of sustained altered compressive loading and its relationship to the initiation of degenerative changes to the tibio-femoral joint. The VLD applies decreased compressive load to the lateral compartment and increased compressive load to the medial compartment of the tibio-femoral joint in a controlled manner.
Mature rats were randomized into one of three groups: unoperated control, 0% (sham) or 80% body weight (BW). Devices were attached to animal’s leg to deliver altered loads of 0% and 80% BW to the experimental knee for 12 weeks. Compartment-specific material properties of the tibial cartilage and subchondral bone were determined using indentation tests. Articular cartilage, calcified cartilage and subchondral bone thicknesses, articular cartilage cellularity, and degeneration score were determined histologically.
Joint tissues were sensitive to 12 weeks of decreased compressive loading in the lateral compartment with articular cartilage thickness decreased in the peripheral region, subchondral bone thickness increased, and cellularity of the midline region decreased in the 80% BW group as compared to the 0% BW group. The medial compartment revealed trends for diminished cellularity and aggregate modulus with increased loading.
The rat-VLD model provides a new system to evaluate altered quantified levels of chronic in vivo loading without disruption of the joint capsule while maintaining full use of the knee. These results reveal a greater sensitivity of tissue parameters to decreased loading versus increased loading of 80% BW for 12 weeks in the rat. This model will allow future mechanistic studies that focus on the initiation and progression of degenerative changes with increased exposure in both magnitude and time to altered compressive loads.”
” The VLD applies altered loads in addition to the normal loads across the joint without disruption of the joint capsule while maintaining full use and range of motion of the joint.”
The mice were 9-month old sprague dawley. The rats had the plates attached surgically so it’s not really an exact approximation of LSJL. And the 0% BW results were drastically different from control so the apparatus definitely had an effect.
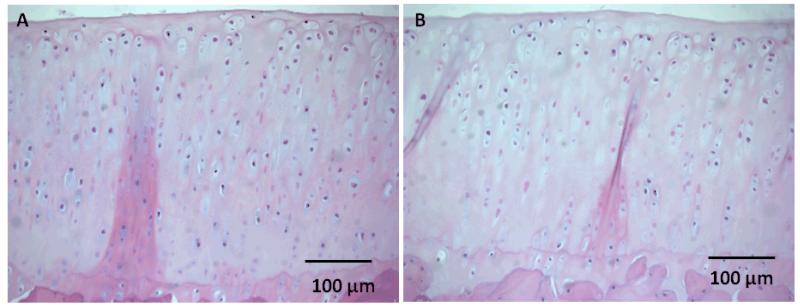
“Gross observation of the tibial plateau revealed minimal erosion or fibrillation of the articular cartilage in all experimental groups.”
“The thickness of the articular cartilage in the peripheral region of the lateral compartment decreased 19% in the 80% BW group as compared to the 0% BW group and 26% as compared to the control group. In contrst, the thickness of the subchondral bone increased 38% in the 80% BW group as compared to the 0% BW group”<-So loading increases subchondral bone “thickness” but does this thickness add to height?
Here’s a comparison between sham control(0% BW) and 80% BW. Loading definitely decreased chondrocyte number but it didn’t seem to decrease articular cartilage height and subchondral bone height seemed to be higher.
Short and tall stature: a new paradigm emerges.
Full Study->jeffreybaron study
“In the past, the growth hormone (GH)-insulin-like growth factor 1 (IGF-1) axis was often considered to be the main system that regulated childhood growth and, therefore, determined short stature and tall stature. However, findings have now revealed that the GH-IGF-1 axis is just one of many regulatory systems that control chondrogenesis in the growth plate, which is the biological process that drives height gain. Consequently, normal growth in children depends not only on GH and IGF-1 but also on multiple hormones, paracrine factors, extracellular matrix molecules and intracellular proteins that regulate the activity of growth plate chondrocytes. Mutations in the genes that encode many of these local proteins cause short stature or tall stature. Similarly, genome-wide association studies have revealed that the normal variation in height seems to be largely due to genes outside the GH-IGF-1 axis that affect growth at the growth plate through a wide variety of mechanisms. These findings point to a new conceptual framework for understanding short and tall stature that is centred not on two particular hormones but rather on the growth plate, which is the structure responsible for height gain.”
Note extracellular fluid is listed as a factor and extracellular fluid flow can be modified by LSJL.
“the vast majority of children with short stature do not have a well-substantiated defect in the GH–IGF-1 axis.”
“Many new genes have been identified that, when mutated, result in short stature or tall stature, the majority of which do not participate in the GH–IGF-1 system”
“Estrogen has complex effects on the growth plate, not only altering growth rate, but also accelerating the loss of progenitor cells in the resting zone and thereby speeding up the developmental program of growth plate senescence, which causes early cessation of growth”
“tumour necrosis factor, IL-1β and IL-6 act directly on growth plate cartilage to suppress bone growth”
“fairly low doses of ionizing radiation, such as a single dose of 10 Gy, can impair longitudinal growth. Mechanical compression across the growth plate also impairs the elongation of bones, which is partly due to decreased enlargement of hypertrophic chondrocytes.”<-Chondrocyte hypertrophy size increases due to lsjl.
“FGFR-3 signalling negatively regulates growth by decreasing proliferation in the proliferative zone, decreasing production of the extracellular matrix, accelerating the onset of hypertrophic differentiation and decreasing the size of the hypertrophic chondrocytes”
“~2% of children who present with idiopathic short stature have mutations in NPR2, Conversely, overexpression of CNP or activating mutations in NPR2 result in tall stature.”
” Binding of CNP to NPR2 stimulates the guanylyl cyclase activity of the receptor, thereby increasing synthesis of cGMP, which activates the type II cGMP-dependent protein kinase”
“Of individuals presenting with idiopathic short stature, 2–15% have mutations in SHOX, with the exact percentage depending on the study. Conversely, increased copies of SHOX are associated with tall stature in individuals with Klinefelter syndrome and other types of sex chromosome aneuploidy”
“Sotos syndrome (characterized by tall stature) is associated with decreased activity of the Ras–MAPK pathway.”
“Ras, a small GTPase, signals via MAPK cascades to phosphorylate numerous cytoplasmic and nuclear proteins, regulating cell proliferation and differentiation.”
“heterozygous mutations in DNA methyltransferase 3A (DNMT3A) cause tall stature, a distinctive facial appearance and intellectual disability.”
“heterozygous mutations in EZH2, which encodes an enzyme that specifically methylates lysine residue 27 of histone 3 (H3K27, which is associated with transcriptional repression), are associated with Weaver syndrome (characterized by prenatal and postnatal overgrowth and a markedly advanced bone age).”
There’s a lot more covered in the study than I mentioned here. The full study is worthwhile to read.
It’s frustrating how much bodybuilding research there is in terms of sets, reps, and all sorts of factors to build up muscle and how little there is in terms of height. Note that most of this research does not come from science it comes from tons of independent bodybuilders.
With muscle building we know that stressing the muscles in general increases their size. Bodybuilders don’t wait for calf and pec implants to get bigger muscles.
We don’t know though how to lengthen bone? We don’t know what stimulus to apply? Actually we have a pretty good idea.
To induce chondrogenic differentiation(chondrocytes are the basis for the growth plate) one method is to induce a hydrostatic pressure of at least 0.1 MPa. A blood pressure cuff during a heart beat generates about 120mmHg which is about 0.015MPa an order of magnitude of what we need. To get 0.1MPa we’d need a blood pressure of about 750mmHg which would probably cause death. There has to be a way for the body to safely induce hydrostatic pressure of 0.1MPa-10MPa’s to induce chondrogenic differentiation. HP levels of the articular cartilage can vary between 1-5MPa in response to physiological(occurs normally) stress. There are two possible ways to make up the difference in the hydrostatic pressure deficit(0.015MPa versus 0.1MPa or ideally higher) fluid flow and bone deformation.
Ultrasound levels of 30–200 mW/cm2, Frequency=1–1.5 MHz are one possibility(you’d target in the epiphysis). Note I have not tested this so attempt at your own risk! Muscular contraction can also increase marrow hydrostatic pressure. You’d probably need to use external electrical stimuli to generate the muscular contraction needed to induce significant hydrostatic pressure. Again I can not say whether or not this is safe or not!
An increase in hydrostatic pressure also results in an increase in fluid flow which may be the primary inducer of chondrogenic differentiation rather than the HP itself. Thus you could find ways to induce fluid flow directly and in conjunction with an increase in hydrostatic pressure to get the needed stimulus to induce chondrogenic differentiation.
The growth plate is exposed to high hydrostatic pressure via the bone pressing down on it. If we create a fibrous layer in a neo-growth plate region maybe the hydrostatic pressure to encourage a growth plate will occur naturally. Note that LSJL does encourage fibrous tissue differentiation. If we can create a fibrous tissue layer, the compression force of the bone itself will create the hydrostatic pressure and induce chondroinduction.
So we know the key to growing taller is to induce a new growth plate in the bone as bone tissue is not mechanically suited for interstitial growth. We know that this can happen at around 0.1MPa hydrostatic pressure in the bone epiphysis. It’s possible to make up for a deficit in hydrostatic pressure levels via other factors like fluid flow via dynamic lateral compression. There’s also the possibility of using ultrasound and electrical muscle stimulation. Such levels would have to be supranormal as no muscle stimulation of longitudinal bone growth has yet to be reported. Since it is supranormal all the effects are not known so it would have to be tested somewhat for safety first.
Metformin Hydrochloride is used to treat type II diabetes. It’s possible that Metformin could increase height via a SIRT1 cellular senescence related mechanism, a mitochondrial related mechanism(chondrocytes are hypoxic so metformin could affect height in that way), or another mechanism.
Evaluating the Effects of Metformin Use on Height in Children and Adolescents: A Meta-analysis of Randomized Clinical Trials.
“Metformin hydrochloride use is increasing in children and adolescents. [There’s] a large variability in the effects of metformin use on body mass index changes but have not considered height changes as a confounder{Height affects BMI, Metforim may affect height}.
To conduct a systematic review and meta-analysis of the effects of metformin use on height in children and adolescents.
Computerized databases, including MEDLINE and EMBASE, were searched up to September 9, 2014, for terms related to metformin and childhood or adolescence.
Randomized clinical trials examining the effects of metformin use on height of participants younger than 19 years were considered eligible. Trials with cointerventions other than lifestyle changes were excluded.
Height, weight, body mass index, age, sex, metformin dosage, and study duration were independently extracted by 2 reviewers. The weighted mean differences for changes in height, weight, and body mass index were compared between the metformin and control groups using random-effects models.
Ten studies were included, with a total of 562 participants, 330 (58.7%) of whom were female. The mean age within the studies ranged from 7.9 to 16.1 years, with a high variability in most studies. The duration of metformin interventions lasted from 3 to 48 months. Overall, height changes were not significantly different between the metformin and control groups. However, stratified analyses according to the cumulative metformin dose (in milligrams per day times the number of days of treatment) showed a greater increase in height with metformin use in the 5 studies providing the largest cumulative metformin doses (weighted mean difference, 1.0; 95% CI, 0.0 to 2.0 cm) but not in the 5 studies providing the lowest doses (weighted mean difference, -0.1; 95% CI, -0.7 to 1.0 cm) compared with the control group.
Preliminary evidence suggests a dose-response relationship between metformin use and increases in height in children and adolescents compared with a control group. While an approximate 1-cm increase in height may appear small, it is likely underestimated given that many studies were of short duration and included older adolescents, potentially after epiphyseal growth plate closure.”
Metforrim may have had an impact on height by up to 2cm in subjects that high doses of metforrim.
“A greater cumulative exposure to metformin may increase height by a mean of approximately 1 cm in children and adolescents compared with a control group.”<-A dedicated study is needed though.
“a 2.8-cm greater increase in height in the metformin group for girls approximately 9 years old”
“metformin administration during puberty could enhance or prolong the normally occurring, puberty induced height change”
Does Metformin Really Increase Height, or Is There Some Problem With the Controls?—Reply
“thank Poulton for the thoughtful letter that stated that the greater increase in height observed in studies from our meta-analysis with the highest cumulative metformin dose was owing to “a combination of inaccurate and abnormally slow growth rates in the control individuals.”
We agree that artifacts could arise from a higher attrition level in the study by Kendall et al, and understand why it is tempting for Dr Poulton to suggest that we should reanalyze without this study. However, we disagree that we should exclude an individual study owing to its attrition level without applying this criterion to all studies (eg, the study by Mauras et al had the highest control group attrition rate but a −0.2-cm change in height in the metformin vs the control group). While the changes in height in the control group from Kendall et al (ie, 1 cm in 6 months; mean baseline age of 13.6 years) may seem “suspiciously slow,” it is not dissimilar from other studies we reviewed that were comparable in terms of duration and participants’ baseline age. This “slower growth than normal in the controls” may therefore be explained by findings that suggest children with obesity have an earlier peak height velocity and onset of puberty, but lower peak height velocity. For these reasons, we believe it would be inappropriate for us to single out and exclude the data from Kendall et al.“
Early metformin therapy to delay menarche and augment height in girls with precocious pubarche
“At age 8 years, girls were randomly assigned to remain untreated or to receive metformin for 4 years; subsequently, both subgroups were followed without treatment until each girl was postmenarcheal.
Age at menarche, height, weight, endocrine-metabolic state (fasting blood), body composition (by absorptiometry), abdominal fat (subcutaneous vs. visceral), and hepatic adiposity (by magnetic resonance imaging).
At last assessment, girls in each subgroup were on average 2 years beyond menarche; the mean growth velocity was below 2 cm/years. Age at menarche was 11.4 ± 0.1 years in untreated girls and 12.5 ± 0.2 years in metformin-treated girls; the latter girls were taller and much leaner (with less visceral and hepatic fat) and had more favorable levels of circulating insulin, androgens, and lipids.
Early metformin therapy (age ∼8–12 years) suffices to delay menarche; to augment postmenarcheal height”
Metformin for Rapidly Maturing Girls with Central Adiposity: Less Liver Fat and Slower Bone Maturation
“he tempo of bone aging was accelerated in untreated girls (≈16% faster vs. chronological aging) and normal in metformin-treated girls (≈20% slower vs. untreated girls). Metformin-treated girls gained more height per bone-age year and had less visceral and hepatic fat. The tempo of bone maturation was associated (R = 0.55; p < 0.001) with hepatic fat. Metformin treatment in rapidly maturing girls with central adiposity normalized bone maturation. This normalization was accompanied by less central fat and was related closely to hepatic fat.”
Below is a demonstration of me performing LSJL on the femoral epiphysis. The key to chondroinduction as is expanded on below(need to get the studies from UCSD, does anyone have access to them?) is to achieve between 0.1 – 10(or more) MPa in the epiphyseal bone marrow. A blood pressure cuff can achieve 120mmHg during a heart beat which is about 0.015MPa an order of magnitude below what we need. The highest recorded blood pressure is 300mmHg which is still below what we need. Systolic blood pressure is “specifically the maximum arterial pressure during contraction of the left ventricle of the heart.” We’re not specifically looking for the arterial pressure we’re looking for the bone marrow hydrostatic pressure.
The key to distraction osteogenesis may be the blood clot that’s formed during the fracture. This creates a chondrogenic environment. And this fracture does not pose a large risk to health. So the goal is to mimic the hydrostatic pressure creation in the bone marrow without inducing fracture. Note in the video that my knee is bent to increase the pressure.
Nothing much in the video. Just me performing the new LSJL method on my left knee epiphysis. This is exactly the way I do it except I’m usually lying down on my back so it’s easier to perform.
“Skeletal adaptation to mechanical loading is controlled by mechanobiological signaling. Osteocytes are highly responsive to applied strains, and are the key mechanosensory cells in bone. However, many cells residing in the marrow also respond to mechanical cues such as hydrostatic pressure and shear stress, and hence could play a role in skeletal adaptation. Trabecular bone encapsulates marrow, forming a poroelastic solid. According to the mechanical theory, deformation of the pores induces motion in the fluid-like marrow, resulting in pressure and velocity gradients. The latter results in shear stress acting between the components of the marrow. To characterize the mechanical environment of trabecular bone marrow in situ, pore pressure within the trabecular compartment of whole porcine femurs was measured with miniature pressure transducers during stress-relaxation and cyclic loading. Pressure gradients ranging from 0.013 to 0.46kPa/mm were measured during loading. This range was consistent with calculated pressure gradients from continuum scale poroelastic models with the same permeability. Micro-scale computational fluid dynamics models created from computed tomography images were used to calculate the micromechanical stress in the marrow using the measured pressure differentials as boundary conditions. The volume averaged shear stress in the marrow ranged from 1.67 to 24.55Pa during cyclic loading, which exceeds the mechanostimulatory threshold for mesenchymal lineage cells{but we have to be in the range to stimulate chondrodifferentiation}. Thus, the loading of bone through activities of daily living may be an essential component of bone marrow health and mechanobiology. Additional studies of cell-level interactions during loading in healthy and disease conditions will provide further incite into marrow mechanobiology.”
Intermittent hydrostatic pressure can induce chondrostimulation. 0.1 to 10 MPa tend to be the levels to induce chondrogenic differentiation. There are 1 million Pascals in a MegaPascal so the average shear stress in the bone marrow from cyclic loading is below the levels needed to induce chondroinduction. 0.1MPa is needed to induce proteoglycan production and above 10MPa induces more chondrogenic markers.
“Bone adapts to habitual loading through mechanobiological signaling. Osteocytes are the primary mechanical sensors in bone, upregulating osteogenic factors and downregulating osteoinhibitors, and recruiting osteoclasts to resorb bone in response to microdamage accumulation. However, most of the cell populations of the bone marrow niche,which are intimately involved with bone remodeling as the source of bone osteoblast and osteoclast progenitors, are also mechanosensitive. We hypothesized that the deformation of trabecular bone would impart mechanical stress within the entrapped bone marrow consistent with mechanostimulation of the constituent cells. Detailed fluid-structure interaction models of porcine femoral trabecular bone and bone marrow were created using tetrahedral finite element meshes. The marrow was allowed to flow freely within the bone pores, while the bone was compressed to 2000 or 3000 microstrain at the apparent level.Marrow properties were parametrically varied from a constant 400 mPas to a power law rule exceeding 85 Pas. Deformation generated almost no shear stress or pressure in the marrow for the low viscosity fluid, but exceeded 5 Pa when the higher viscosity models were used{high viscosity is high internal friction?. The shear stress was higher when the strain rate increased and in higher volume fraction bone. The results demonstrate that cells within the trabecular bone marrow could be mechanically stimulated by bone deformation, depending on deformation rate, bone porosity, and bone marrow properties{we need to alter this with LSJL}. Since the marrow contains many mechanosensitive cells, changes in the stimulatory levels may explain the alterations in bone marrow morphology with aging and disease, which may in turn affect the trabecular bone mechanobiology and adaptation.”
The higher the temperature is, the lower a substance’s viscosity is. Consequently, decreasing temperature causes an increase in viscosity.
Bone is considered to have laminar flow in that the bones move in separate layers. Bone is a viscous tissue meaning “having a thick, sticky consistency between solid and liquid; having a high viscosity”<-Salt, cornstarch, and flour are ways to increase bone marrow viscosity.
A blood pressure cuff generates 120mmHg ish which is about 0.015MPa. You need about 75000mmHg to generate 10MPa. Specifically we want to increase the intraosseous pressure.
“During rapid dynamic loading, however, a slight rise in intra-medullary pressure was observed. Contraction of the femoral muscles also resulted in a greater bone-marrow pressure increase. A correlation of 0.98 between stimulus strength and intra-medullary pressure was obtained. The rise in intra-medullary pressure with femoral muscle contraction is suggested to have a possible role under extreme stresses in living conditions.”
“The normal resting range of bone-marrow pressure in all the rats studied in the present
series varied from 1.07 to 2.40 kPa (8 to 18 mmHg) [mean resting pressure 1.65 kPa (12.4
mmHg), standard error of the mean 0.08 kPa (0.6 mmHg)]. The most frequently observed
values were between 1.6 kPa to 1.87 kPa (12 to 14 mmHg). The marrow pressure tended
to vary within the range of 0.267 kPa under resting conditions. “<-This is about 3 orders of magnitude of the pressure we need.
“The bone-marrow pressure did not alter [during slow loading] either during the period of loading or on completion of the process and maintenance of the load. ”
“In slow loading experiments the compression was applied over a period of 1 minute to gaps of
1.36 kg from 0 to 12.25 kg by slow rotation of the central loading screw. Each applied load was
maintained for 2 minutes to allow for any gradual pressure build-up. Any rise in the marrow
pressure following loading was permitted to settle before the next incremental load was applied. During fast loading similar loads were applied but the process of each loading was completed within 2 seconds. After each step of loading there was an observational pause of 2 minutes. A sudden loading omitting two and more of the intermediate steps was also tried. ”
“During fast loading, bone-marrow pressure variations were normal within the range of 0
to 2.7 kg. Beyond this level as the loads were swiftly applied, sudden pressure changes were
observed, these being more pronounced if the loading omitted two of the intermediate
steps. A rise of 2 kPa (15 mmHg) was observed when the compression was raised
from 4 kg to 12.25 kg. Generally, a higher magnitude of compression engendered greater increases in the intra-medullary pressure. ”
“Stimulation of the femoral nerve, causing contraction of the quadriceps muscles
resulted in a considerable rise in bone marrow pressure. There was a progressive increase in bone-marrow pressure with each increment in stimulus strength. A maximum pressure rise of 8 kPa (60 mmHg) was recorded with 5 V stimulation.”
“In life, excessive compression stress tends to cause bone fracture which can be resisted by
the sudden and significant rise of marrow pressure caused by simultaneous contraction of the overlying muscles”
This next study found that pressure increased by approximately 3X in response to load which still doesn’t get us up three orders of magnitude:
“Increases in ImP may be induced by deformations in the matrix that result in volumetric decreases in the intramedullary cavity”
“dynamic IFF rather than pressure was the primary factor driving skeletal adaptation in our studies.”<-Perhaps it is the same for inducing chondroinduction?
” in vitro in sheep tibia (up to 300 mmHg in response to a load of 2000 N over 0.15 second) and excised human femurs (93.5 mmHg in response to a load of 980 N over 0.03 second)”
“sinusoidal forces of 0.5 Hz and 10 Hz, pressure amplitude increased up to 4-N loads and reached a plateau at 130 Pa.”<-which is 3 orders of magnitude below where we need to be but maybe it is interstitial fluid flow that can induce chondrogenesis and not hydrostatic pressure.
According to Mechanobiology of mandibular distraction osteogenesis: finite element analyses with a rat model., “A 0.25 mm distraction was simulated and the resulting hydrostatic stresses and maximum principal tensile strains were determined within the tissue regenerate. When compared to previous histological findings, finite element analyses showed that tensile strains up to 13% corresponded to regions of new bone formation and regions of periosteal hydrostatic pressure with magnitudes less than 17 kPa corresponded to locations of cartilage formation. Tensile strains within the center of the gap were much higher, leading us to conclude that tissue damage would occur there if the tissue was not compliant enough to withstand such high strains, and that this damage would trigger formation of new mesenchymal tissue. These data were consistent with histological evidence showing mesenchymal tissue present in the center of the gap throughout distraction.”<-So it is possible to form cartilage with less than 0.1MPa.
” In reality, tensile hydrostatic stresses (i.e., negative pressures) greater than 47.07 mmHg (=6.3 kPa), which is the vapor pressure of water at 37 degrees C, would cause the water in the tissue to boil.”
Pressure in a liquid is the force exerted over a given area, a fluid’s pressure pushes on the walls of the surrounding container, as well as on all parts of the fluid itself.
The pressure in the liquid increases with depth because of gravity. The liquid at the bottom has to bear the weight of all the liquid above it, as well as the air above that.
Here’s a study that states that maybe it’s interstitial fluid flow and not necessarily hydrostatic pressure that can induce changes in bone(and therefore chondroinduction):
“Fluid flow that arises from the functional loading of bone tissue has been proposed to be a critical regulator of skeletal mass and morphology. To test this hypothesis, the bone adaptive response to a physiological fluid stimulus, driven by low magnitude, high frequency oscillations of intramedullary pressure (ImP), were examined, in which fluid pressures were achieved without deforming the bone tissue. The ulnae of adult turkeys were functionally isolated via transverse epiphyseal osteotomies, and the adaptive response to four weeks of disuse (n=5) was compared to disuse plus 10min per day of a physiological sinusoidal fluid pressure signal (60mmHg, 20Hz). Disuse alone resulted in significant bone loss (5.7±1.9%), achieved by thinning the cortex via endosteal resorption and an increase in intracortical porosity. By also subjecting bone to oscillatory fluid flow, a significant increase in bone mass at the mid-diaphysis (18.3±7.6%), was achieved by both periosteal and endosteal new bone formation. The spatial distribution of the transcortical fluid pressure gradients (∇Pr), a parameter closely related to fluid velocity and fluid shear stress, was quantified in 12 equal sectors across a section at the mid-diaphyses. A strong correlation was found between the ∇Pr and total new bone formation (r=0.75); and an inverse correlation (r=-0.75) observed between ∇Pr and the area of increased intracortical porosity, indicating that fluid flow signals were necessary to maintain bone mass and/or inhibit bone loss against the challenge of disuse. By generating this fluid flow in the absence of matrix strain, these data suggest that anabolic fluid movement plays a regulatory role in the modeling and remodeling process. While ImP increases uniformly in the marrow cavity, the distinct parameters of fluid flow vary substantially due to the geometry and ultrastructure of bone, which ultimately defines the spatial non-uniformity of the adaptive process.”
“one is a highly structured composite material comprised of a collagen-hydroxyapatite matrix and a hierarchical network of lacunae-canaliculi channels. These tunnels permit interstitial flow of fluid through tiny microporosities, and thus ‘‘by-products’’ of load, such as the change in fluid velocities or pressures, represent a means by which a physical signal could be translated to the cell{Mesenchymal Stem Cells are cells so could be affected by fluid pressures as well}”
“intracortical fluid flow is induced not only by bone matrix deformation, but also by the intramedullarypressure (ImP) generated during loading. Applying anabolic oscillatory ImP alone can induce transcortical fluid flow as measured by streaming potential”<-So there are two alternatives to achieving 0.1 MPa in the epiphyseal bone marow: oscillitary intramedullary pressure and bone matrix deformation to induce fluid flow.
” maximum fluid pressure on the order of 8 kPa will result in approximately 0.8 [microstrain] in the matrix.”
“While the endosteum is permeable, theyhave found that the periosteum is, in essence, impermeable unless the periosteal superficial layer is removed in the adult canine tibial cortex.”
“Cells continuously receive biochemical and biophysical stimuli from their microenvironment. These environmental stimuli drive cellular behavior and function during development and tissue regeneration.”<-We can alter the microenvironment via mechanical means to alter cellular behavior and ideally create neo-growth plates.
“Cell interactions with the extracellular matrix (ECM) and physical signals such as matrix rigidity and mechanical stimuli can also have strong effects on cellular phenotype and tissue formation.”<-The bone ECM likely has a strong negative regulatory effect on neo-growth plate formation. But we can alter the bone ECM via mechanical means as well.
“[we prepared] HP-ALG hydrogels with incorporated gradients of heparin binding growth factors BMP-2, a potent osteogenic growth factor, and TGF-β1, a chondrogenic growth factor, in opposite directions. When the concentration of growth factors in segments of gradient HP-ALG hydrogels was quantified, linear gradient distributions of BMP-2 and TGF-β1 in opposite directions were observed”
“As the BMP-2 concentration increased, ALP expression significantly increased along the BMP-2 gradient. In contrast, GAG production of encapsulated hMSCs significantly increased as the TGF-β1 concentration increased”
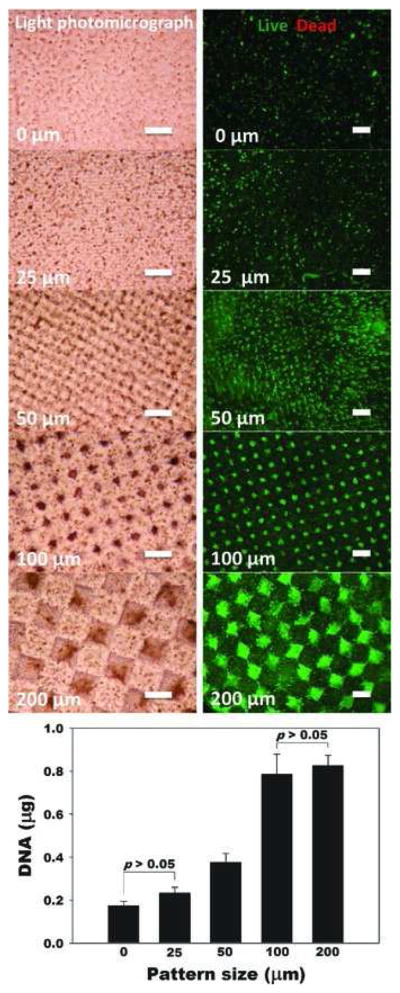
“By manipulating micropattern size while keeping the overall ratio of single- to dual-crosslinked hydrogel volume constant, the physical properties of the micropatterned alginate hydrogels are spatially tunable. When human adipose-derived stem cells (hASCs) are photoencapsulated within micropatterned hydrogels, their proliferation rate is a function of micropattern size. Additionally, micropattern size dictates the extent of osteogenic and chondrogenic differentiation of photoencapsulated hASC. The size of 3D micropatterned physical properties in this new hydrogel system introduces a new design parameter for regulating various cellular behaviors, and this dual-crosslinked hydrogel system provides a new platform for studying proliferation and differentiation of stem cells in a spatially controlled manner for tissue engineering and regenerative medicine applications.”
“cell behaviors such as differentiation and proliferation are known to be affected by cell cluster size”
” micropattern size dictated the extent of osteogenic and chondrogenic differentiation of photoencapsulated hASC.”
“the aggrecan expression of hASCs gradually increased as the micropattern size increased”<-But some markers increased at 200 micrometers so the optimal micropattern size should be around 100-200 micrometers.
“The reconstruction of musculoskeletal defects is a constant challenge for orthopaedic surgeons. Musculoskeletal injuries such as fractures, chondral lesions, infections and tumor debulking can often lead to large tissue voids requiring reconstruction with tissue grafts. Autografts are currently the gold standard in orthopaedic tissue reconstruction; however, there is a limit to the amount of tissue that can be harvested before compromising the donor site. Tissue engineering strategies using allogeneic or xenogeneic decellularized bone, cartilage, skeletal muscle, tendon and ligament have emerged as promising potential alternative treatment. The extracellular matrix provides a natural scaffold for cell attachment, proliferation and differentiation. Decellularization of in vitro cell-derived matrices can also enable the generation of autologous constructs from tissue specific cells or progenitor cells. Although decellularized bone tissue is widely used clinically in orthopaedic applications, the exciting potential of decellularized cartilage, skeletal muscle, tendon and ligament cell-derived matrices has only recently begun to be explored for ultimate translation to the orthopaedic clinic.“
“ECM is a product of cells that functions to maintain tissue and organ structure, organization and function. It is a complex network of proteins and polysaccharides forming an intricate meshwork within tissue that interacts with the resident cells to regulate cell behavior, such as migration, proliferation and differentiation. The ECM exists in a state of dynamic equilibrium with its resident cells and is constantly being built, reshaped and degraded in response to changing environmental conditions and to cellular, tissue and organ demands”<-So we should try to alter the bone ECM to be more favorable to cartilaginous tissues.
“Fracture healing requires an intricate and well-organized series of cellular and molecular events. It involves interactions between cortical bone, the periosteum, undifferentiated fascial tissue surrounding the fracture and the bone marrow. Fracture healing is divided into three stages: inflammation, repair and remodeling. After an injury, there is initial bleeding from the damaged bone ends and surrounding tissue resulting in the formation of a hematoma, which provides a source of hematopoietic cells capable of secreting growth factors. The invasion of inflammatory cells, fibroblasts, mesenchymal cells, and osteoprogenitor cells at the fracture site forms granulation tissue around the fracture ends{To induce neo-growth plates we have to allow this invasion}. Fractures that are anatomically aligned with absolute stability, such as those surgically repaired with compression plates, undergo primary bone healing or Haversian remodeling, in which there is direct osteonal healing within the cortex by intramembranous ossification”
” in closed reduced fractures, secondary bone healing occurs with the formation of a bridging soft callus consisting of cartilage tissue connecting the fracture ends. Over time, bone formation occurs under the periosteum and calcification of cartilage results in the formation of hard callus or woven bone by endochondral ossification”
“injuries that penetrate the subchondral bone often result in the formation of fibrocartilage which is biomechanically insufficient compared to hyaline cartilage, resulting in further damage over time”
“the peak force transmitted through the Achilles tendon while running is 9 kN, which is about 12.5 times the body weight”

 Note extracellular fluid is listed as a factor and extracellular fluid flow can be modified by LSJL.
Note extracellular fluid is listed as a factor and extracellular fluid flow can be modified by LSJL.