In the previous post I offered proof that my current LSJL was working for my fingers(and reported anecdotal evidence of increasing my wingspan by a couple of inches without photographic evidence) but that the LSJL method for the legs was lacking. So I’m revising the LSJL method to be more like what I’m doing for the fingers which I’ve gotten gotten results from. With an emphasis on intensity rather than duration. If anyone has any ideas on how to get a more intense clamp please suggest them. This is only for people with closed growth plates, people with open growth plates should clamp similarly but much lighter as there is no need to try to use clamping to create a more favorable microenvironment for cartilage growth.
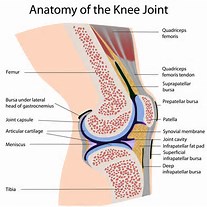
You want to clamp on the synovial joint between the tibia and femur. Michael has suggested that you should load lower on the epiphysis rather than above. However, I think loading the synovial joint is important. The bone there is weaker and it’s easier to cause deformation of the synovial joint then it is the bone itself. There might be stimulus from the synovial joint that stimulates neo-growth plate formation. The synovial joint is connected to the growth plate area after all. You want to clamp more on the femur than the tibia as the clamp will eventually slip to be closer to the middle. You always want to start clamping more on the bigger bone so it slips to the middle. If it slips to be clamping on one bone then restart. Essentially: Make sure you are clamping the synovial joint.
 Now you want to use the Irwin Quick Grip(Irwin Industrial Tools 512QCN Next Generation 12-Inch Clamp and Spreader
Now you want to use the Irwin Quick Grip(Irwin Industrial Tools 512QCN Next Generation 12-Inch Clamp and Spreader). But any clamp that can generate enough pressure is sufficient as long as it avoids slipping. Try to clamp as hard as possible. Use both hands to get harder clamps. Take breaks with the clamp still on and the pressure still applied and try to clamp harder. This method is untested so I can not make any guarantees on the optimal pressure nor can I guarantee that you won’t suffer an injury. Right now my goal is to generate enough pressure such that there’s a visual or feeling of increased blood flow. The goal is to generate hydrostatic pressure to create a pro-chondrogenic microenvironment to encourage new growth plate formation. With my fingers I could see visually increased blood flow and I could feel it. The goal is to generate enough pressure in the synovial joint to encourage a pro-chondrogenic microenvironment. Any clamping method that does that is sufficient.
Here’s another angle:

Me clamping between the tibia and talus:

Me clamping between the talus and calcaneus:

Please let me know if you have any questions. I know people will want a video so I’ll work on that for Part III.
Michael: Here is what I would suggest. Get a 2nd clamp to clamp simultaneously for the knee area. We do have two hands, and the clamping area is on the legs. A easy position to get into. To get the frequency correct, squeeze both hands at the same time.
Fit the two clamps along side of each other, one on the angular part while the other is on the sides, which you suggest. Since load is just pressure (Force/area) to increase the load, we just get a 2nd clamp to double the amount. At this point, I would not suggest increasing the amount of force from one clamp, but put the clamps into series on the sides of the tibia.