This is probably the first really long post I have written in maybe 2 months. However, there have been an accumulation of new evidence suggesting that for some people even in their mid-20s, after full epiphyseal growth plate closure, could notice height increases, but at a smaller level.
This is probably the first really long post I have written in maybe 2 months. However, there have been an accumulation of new evidence suggesting that for some people even in their mid-20s, after full epiphyseal growth plate closure, could notice height increases, but at a smaller level.
So why do I now believe in this theory which goes against everything that the medical literature claims?
The first thing is that I have finally gotten around to reading this book “Bones and Bones, 2nd Edition” by Weinmann and Sicher for the last 4 months on my desk which I only cracked a few times. Tonight I took a really close look at what the medical authors wrote in the section on abnormal pituitary stimulation causing gigantism and acromegaly.
From page 210 to 228, the focus was on the overproduction of hGH from the pituitary gland. The stuff on Gigantism wasn’t too helpful, but the stuff written about Acromegaly was.
If the readers would ever buy the book, on page 214 I quote the following sentences….
“The elongation of the hands and feet is often first noted by the patient since he is forced to buy larger gloves and shoes….Probably the fact that each digit in the hand and foot consists of four segments (three in the thumb and big toe) is responsible for the considerable lengthening of the digits by small increments at the articular ends”
“Although increased endochondral ossification of the articular cartilages cannot contribute significantly to the length of the humerus, femur, or similar long bones, an accumulation of small increments on seven sites on the three-phalangeal digits will result in marked elongation…”
The authors would then go on to notice that the excess of HGH in adulthood would cause the thorax area of the chest to become distorted, since in the adult human, the thorax/chest area is still fibrocartilage. HGH can make even fibrocartilage get wider/go into hypertrophy.
As for the irregular vertebral bones, the HGH release causes the bones to grow thicker, growing periosteally, on the anterior and lateral sides.
Along with the bones, the discs between them also get wider.
However, the fibrocartilage next to the discs differentiates, especially at the periphery of the disc and adjacent to the bone, into hyaline cartilage!
As the author, says “Thus, a new site for endochondral ossification is established, which creates a spur and a shelflike hyperostosis at the edges of the vertebral bodies.” Of course, we need to realize that they are talking about bone growth in the horizontal direction, not vertical. However, that doesn’t mean that there is no stimulation for the hyaline cartilage to also push against gravity in the vertical direction.
The last thing to realize is that for people who suffer from acromegaly, their mandible jaw bone over time starts to grow and become longer. That is because of the synovial joint in the area which the zygomatic cheek bone bridge meets the temporal bone with the mandible That is known as the Temporal-Mandibular Joint, or the TMJ. On a related note, it seems that the surgery of limb lengthening is done quite often to the TMJ area to make it longer (why, I don’t know)
So here is what the reader should take away. The following points…
- Even after the long bones have no “growth plates”, growth will still be going on everywhere else, including even the organs inside the body.
- Acromegalic people notice that their fingers and feet seem to get wider and longer, similar to how pregnant females notice the same thing
- The fibrocartilage in their IVD area changes into hyaline cartilage!
- The slight bit of articular cartilage also starts to go into over-activity.
- When it comes to fingers, they will continue to get wider and longer
- The TMJ jaw area of the person which never ossifies slowly makes the person’s skull “longer”
What is most surprising to me is the statement made that the fibrocartilage tissue differentiates into hyaline cartilage! And also remember, that between the fibrous and collagenous type of tissue in the discs and the vertebrate bone, there will always be a very, VERY thin layer of hyaline cartilage tissue, usually only at the thickness of say 3-5 cells across.
Now, let’s take a look at a well known case of a person who became tall due to overactive pituitary gland function. Anthony Robbins. He recently did a video interview with Lewis Howes to promote his first new book in 25 years, dealing with Money, Investing, and how to take control of one’s finances. I clipped one picture from their interview (to see the interview, Click Here).
While I was listening to the interview, I couldn’t help noticing how much bigger Robbin’s head was compared to Lewis’s. Lewis is probably around 6’5″- 6’6″ and Tony is well known for being 6′ 7″. However, Tony doesn’t look proportional. His skull, his upper chest/torso area, and his hands are abnormally large, but the length of his femur/upper leg is disproportionally short. Lewis in comparison looks very proportional.

This reveals (and validates) something which I have theorized for a long time, but may never be proven.
I don’t know anything about Anthony Robbin’s biological father, but I would say that he was not genetically not pre-programmed to end up super-tall, unlike Yao Ming or Shaq, who had tall parents and grandparents. He said he was only 5′ 2″ as a 15 year old kid. The HGH that caused his body to grow seemed to really make his head, torso, and hands, and feet bigger.
That means that when it comes to the long bones, the effect they have didn’t do as much as to the irregular bones.
I remember once theorizing that the disproportionate torso/leg ratio of Michael Phelps was because of his eating habits. For a person who ate a lot as a kid, their torso/leg length ratio would increase.
Now, compare that to a person who was not a big eater as a kid, but still ended up tall, like most NBA players. NBA players are notoriously well known for being “long” which means that their legs, and their arms are super-long, compared to their height. If you look at an old interview with Yao Ming and Tracy McGrady together, you would notice that Yao is 1 foot taller than Tmac when sitting down. That means that for a person like Yao, his height came from his torso mostly, which explains why Yao was known for abnormally short arms, with a wingspan of only 7’4″-7’4.5″. For Yao, his limbs were short.
So I will reiterate my theory again.
- People who are genetically pre-programmed to be tall get their height from their long limbs (arms and legs)
- People can change their pre-programming a little to become taller as adult by eating a lot as a kid, to change the length of their torso relative to the length of their legs, which are more or less set by the height of their “genetics”
Now I am not saying that Robbins was a big eater when he was younger. He probably wasn’t since he lived in a very poor family. His height came from this “gift from god” or stupid luck.
Of course, when it comes to Gigantism, I could play Devil’s Advocate and show another case, Elisany Da Silva, who would attribute her height from the lengthening of her limbs, not her torso. However, I would counter-argue that the proportionality is determined by the age at which the onset of overactive HGH started.
Getting back to the subject, I once wrote a post here on Maurice Tillet, the French Angel, who was actually quite short (5’6″ maybe) but developed acromegaly. The argument I made back then was that Tillet didn’t get any taller even though HGH was overactive in his system, to show that HGH stimulation after growth plate closure was not possible. Now, I am reversing my opinions, but only to show that there are exceptions to the rule. However, I suspect that his acromegaly started later in his life. There is a time limit for when HGH is no longer effective, and it is not at the point of growth plate closure, but some time after it.
Why would I claim this idea? Well, the body of a 30 year old and a 23 year old is very different. I suspect that even at the age of say 24 or 25, even after the growth plates are supposedly “closed” a person who gets a high enough HGH stimulation would find that they would be able to increase their height, but only by as much as 1-1.5 inch though.
The human body is not a fixed entity, similarly to a bone. It is possible to shake the body to made certain biochemical physiological processes to accelerate enough to cause dramatic changes in the body. The very fact that my own girlfriend of the last two years would say that she grew 1 cm makes me wonder whether the human body is capable of making much more dramatic changes in a short period of time.
If the person is young enough, a high enough HGH injection into the body would shock the body into vertical growth for the last time.
It would stimulate the following areas of the body to grow…
- The fibrocartilage in the region of the IVDs would differentiate into hyaline cartilage.
- The 2 very thin layers of hyaline cartilage sandwiched between the discs and the vertebrate bone will start to proliferate just a little.
- The irregular shaped bones in the feet will grow periosteally, have the macroscopic effect of pushing the overall skeletal system upwards, thus grow taller.
- The layer of articular cartilage in the hip joint will increase as well, as well as the articular cartilage of the tibia and femur in the knee joint.
All of the following physiological processes would accumulate in millimeters until the person gets maybe an overall 1 inch of extra height. That is not a lot, but it does prove a concept. The articular cartilage layer will indeed start to get thicker if you get the growth hormone into the system.
If the person needs even more indication that articular cartilage growth is going to contribute to bones lengthening, realize this…
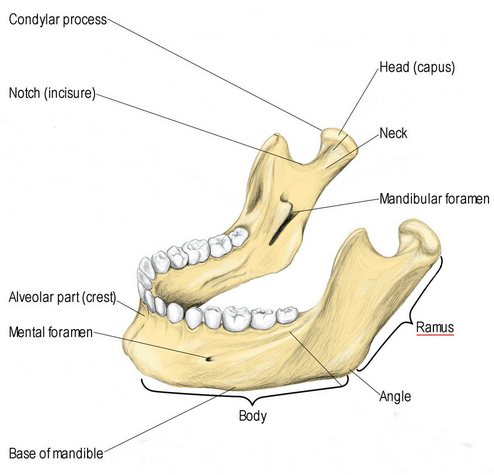
 The mandible grows by endochondral ossification at the condyle and by surface apposition in certain areas. The condylar growth increases the height of the ramus and the overall length of the mandible!!
The mandible grows by endochondral ossification at the condyle and by surface apposition in certain areas. The condylar growth increases the height of the ramus and the overall length of the mandible!!
What that means is that for the human who has his/her normal growth plates closed, and they are have GH overstimulated, thus develop the medical condition known as acromegaly, the condylar growth, which is only from an articular cartilage layer, is enough to increase the length of the ramus, which is just the outer posterior lateral section of the mandible!!
This would suggest that if we could get off of our feet, and into an environment of lower gravity, HGH would work in increasing the length of the much bigger long bones like the femur trough articular cartilage layer deposition. If we were able to lie down on a horizontal bed for 24 hours for maybe 3-4 years, or live in a spaceship with 0 G, our long bones would grow longitudinally, at least up to a noticeable amount.
Concluding statement – Finally, let me reference page 220 of the book, the first paragraph “In acromegaly, growth of the mandible can again be initiated and continued even at a time when growth has normally ceased because of the peculiar histologis structure of the condyle. Here, the bone in younger individuals is covered by a cap of hyaline cartilage, which in turn, is covered by a thick layer of fibrous tissue. Remnants of the hyaline cartilage, which serves as a site of growth in the same way as the epiphyseal cartilage of the long bones, persist even in old individuals. As long as this hyaline cartilage is present, its proliferation can again be set in motion by a hyperactive pituitary gland, and it will then assume its function as a growth center of the mandible where it left off at the termination of normal growth. But even in cases in which an eosinophil adenoma or the hypophysis develops after the disappearance of the cartilaginous cap, a differentiation of hyaline cartilage from the fibrous covering of the condyle is not only possible, but also highly probably. If a new layer of hyaline cartilage has developed, endochondral growth can again set in after resorption of the terminal plate. As in other bones, the periosteal appositional growth is stimulated by the growth hormone; but this growth does not keep pace with the endochondral condylar growth, and the effect is a gradual increase in the mandibular angle.”
What the above paragraph shows is that you can make a bone longer even with just a cap of articular hyaline cartilage, similarly to how the antlers of deers grow out, which I did research more than 2 years ago. The key is to not be pushing down on the cartilage cap, which is not possible since we humans must walk. If we were upside down or had our overall weight lifted from the knee cap cartilage, the tibia bone will most likely start to slowly get longer.
Tyler’s Notes:
Here’s some hand xrays from an acromegalic hand:

First, notice how white it is indicating very high levels of bone density. The epiphysis is much wider than normal.
Here’s another acromegalic hand xray:
 The bones are again much whiter than normal indicating increased density but the increase in epiphyseal width isn’t there.
The bones are again much whiter than normal indicating increased density but the increase in epiphyseal width isn’t there.
Here is another acromegalic hand xray more like the first:

There is epiphyseal widening but not as extreme as the first xray.
Let’s look at some developing fingers:

You can see that not only is the growth plate region not fully developed but the articular end without the growth plate too. It is possible that this development which could occur with physical stimulation or with elevated HGH due to acromegaly could continue into adulthood and contribute to longitudinal bone growth.

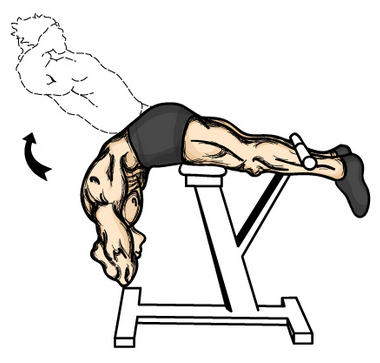 Here is something that I recently found which will help a large percentage of people which will let them gain about half a centimeter in increase height quite quickly. Something which I have always believed is that getting exercise which can remove the load on our backs and vertebrate bone will lead to some height increases.
Here is something that I recently found which will help a large percentage of people which will let them gain about half a centimeter in increase height quite quickly. Something which I have always believed is that getting exercise which can remove the load on our backs and vertebrate bone will lead to some height increases.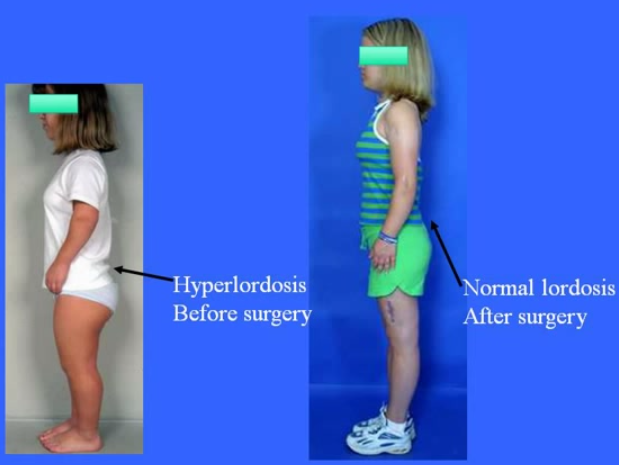 Refer to the Youtube Video “Achondroplasia A Guide For Parents By Dr Dror Paley.mp4”. Notice how the lower back area is curved towards the posterior direction.
Refer to the Youtube Video “Achondroplasia A Guide For Parents By Dr Dror Paley.mp4”. Notice how the lower back area is curved towards the posterior direction.