Articular Cartilage At The End Of Epiphysis Do Growth Thicker Making Bones Longer
I realize that these days I post so little but when I find something very interesting I still make a really good post. This news might really give you guys so really good hope!
 So recently I stopped by a large bookstore in the Gangnam area of Seoul. I had casually mentioned to my girlfriend that I do a lot of medical research and flirted with the idea of maybe one day going to medical school, just for the experience of challenging my intellect. She seemed to be very attracted to the idea of her potential future husband possibly being a doctor and really nudged me towards getting a book that all medical students read, which is a standard anatomy & physiology book. So I scoured the bookshelves looking for something reasonably priced and picked up the a University Level Biology Book “Seeley’s Anatomy & Physiology, 9th Ed. (International Student Edition)“. You can see my iphone picture of it to the right.
So recently I stopped by a large bookstore in the Gangnam area of Seoul. I had casually mentioned to my girlfriend that I do a lot of medical research and flirted with the idea of maybe one day going to medical school, just for the experience of challenging my intellect. She seemed to be very attracted to the idea of her potential future husband possibly being a doctor and really nudged me towards getting a book that all medical students read, which is a standard anatomy & physiology book. So I scoured the bookshelves looking for something reasonably priced and picked up the a University Level Biology Book “Seeley’s Anatomy & Physiology, 9th Ed. (International Student Edition)“. You can see my iphone picture of it to the right.
I decided to peruse through the book to see what they had to say about the epiphyseal growth plate cartilage and how the bones in the body grow. I am already very familiar with how the long bones go through periosteal bone growth, appositional growth, longitudinal growth, and endochondral ossification. However there was a very interesting section which really jumped out at me. On page 186 of the textbook, right underneath a diagram showing the standard defined zones of the epiphyseal plate, there was just 1 paragraph dedicated to the fact that the articular cartilages at the end of bones, long and short, seem to contribute to the volumetric size of the bone!
I took the liberty to take a picture of the section and pasted it below…
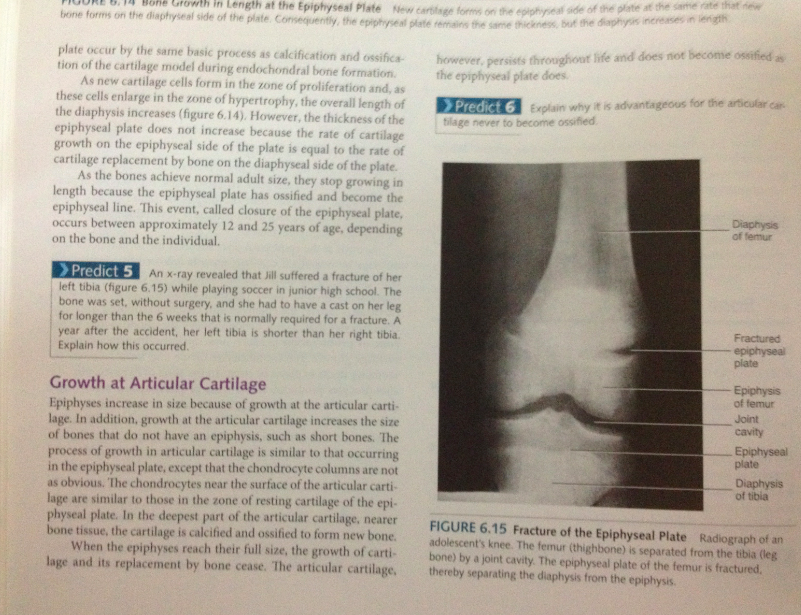
I am not sure whether the reader can read what the section says but here are the main points on the paragraph…
1. The epiphysis does increase in volumetric size from growth of the articular cartilage.
2. Articular cartilage increase the size of bones without even an epiphysis
3. How the articular cartilage makes the bones around it grow in size is similar to how longitudinal growth in the normal growth plates are done.
4. It seems that the chondrocyte columns that is easily seen in any histological examination of the epiphyseal growth plates also exists in the articular cartilage, but they are not as ‘obvious’, whatever that means.
5. It seems that the chondrocytes which are on the surface of the articular cartilage is just like the mesenchymal stem cells which are the progenitor cells which differentiate into the chondrogenic lineage found in the resting zone of the growth plates.
6. When the epiphysis reaches what is supposed to be a maximum size (whatever that may be), the articular cartilage seems to stop its appositional-like growth.
What this proves is that apparently the articular cartilage does contribute to the length of long bones by making the ends of the long bones, the epiphysis larger in size!
They do this just like growth plates.
So the obvious questions to ask then is…
1. Why does the epiphyseal cartilage disappear while the articular cartilage stays for life?
2. Why does the articular cartilage stop producing more bone underneath it after a certain age?
3. Shouldn’t the articular cartilage still have some bit of chondrocytes in it in column-like alignment which could possibly start to hypertrophize and make the bones slightly (1-2 mm) longer?
Answer to Question #1: We answered the first question in an older post Why Does The Epiphyseal Cartilage Disappear But The Articular Cartilage Remain? (Breakthrough!). The answer is that articular cartilage has the SOX9 gene activation the SOX9 Protein and the presence of the Chondromodulin Type 1.
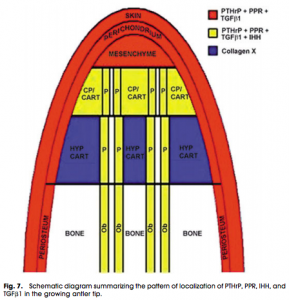 Answer to Question #2: I am going to propose a very good guess on this. When I wrote the post on the analysis of deer antlers Increase Height And Grow Taller From Deer Antler Regeneration Principles, and how they grow biannually, we saw that the structure at the very tip of the deer antler had a mesenchyme reservoir. This is what I would guess the articular cartilage sort of has. The human body has a limited number of mesenchyme close to the surface of the articular cartilage which will slowly over time differentiate into chondroblasts, and then into chondrocytes, and sort of align themselves in some type of columnar fashion.
Answer to Question #2: I am going to propose a very good guess on this. When I wrote the post on the analysis of deer antlers Increase Height And Grow Taller From Deer Antler Regeneration Principles, and how they grow biannually, we saw that the structure at the very tip of the deer antler had a mesenchyme reservoir. This is what I would guess the articular cartilage sort of has. The human body has a limited number of mesenchyme close to the surface of the articular cartilage which will slowly over time differentiate into chondroblasts, and then into chondrocytes, and sort of align themselves in some type of columnar fashion.
When the human being reaches past a certain age, the mesenchyme reservoir gets completely used up. There is nothing left.
Answer to Question #3: I think that there is not enough chondrocytes or mesenchyme left on the inner size of the articular cartilage surface. There might be a few, and there might be ways to get the chondrocytes to hypertrophize, but there is just not enough and there is no way to get the few left to organize themselves in column fashion.
Conclusion:
This new discovery is very, VERY Promising. If the articular cartilage, which is supposed to always exist throughout life, except for maybe certain arthritic cases, does make any type of contribution towards the overall length of long bones, then we have many tools (growth factors like BMP-7 and chondrocyte aligning and regulation signalling factors like thyroxine) already to possibly alter it in certain minimally invasive approaches to get it to start to thicken again and get chondrocytes to multiple in the cartilage.
If we can make the surface of the articular cartilage get some extra mesenchyme, which I theorize is how it originally contributes to the overall size of the epiphysis, then it will start to thicken again, and the chondrocytes on the surface will slowly seep down by diffusion through the cartilage extracellular matrix of Glygoaminoglycans, Proteoglycans, and Collagen Type II, until they form columns. Eventually the diffusion rate of the chondrocytes will slow down, and the chondrocytes will start to form into column-like shapes. I imagine it like how rain water droplets fall slowly into molasses, and the droplets eventually go back into the spherical form due to maximization of the strength of the Force of the Surface Tension. The rain droplets gets trapped at some level, and the result are rain droplets/ chondrocytes stacking along top of each other…
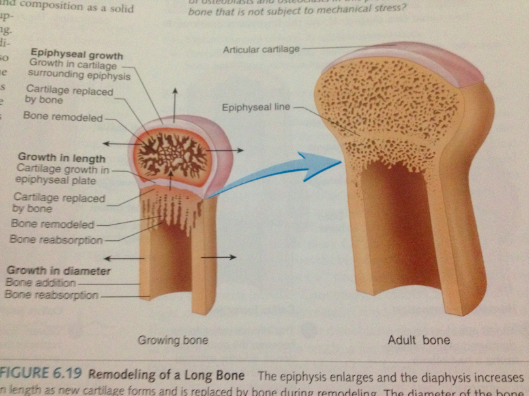
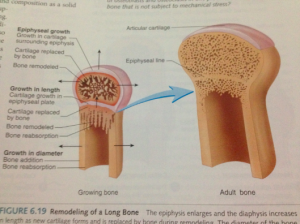 Just look at the picture I took from page 189 of the same textbook. See how the shape and location of the articular cartilage is almost flat and looks very much like half of a full growth plate. It does not enclose around half of the entire epiphysis like it is drawn in some medical school anatomy textbooks. It just sits on the top of the bone. And this is for an adult bone!
Just look at the picture I took from page 189 of the same textbook. See how the shape and location of the articular cartilage is almost flat and looks very much like half of a full growth plate. It does not enclose around half of the entire epiphysis like it is drawn in some medical school anatomy textbooks. It just sits on the top of the bone. And this is for an adult bone!
So all that we have to do to get the articular cartilage to start to deposit bone tissue on the cortical bone layer below it is to get more mesenchyme above it! Of course the obvious joint we are talking about is the knee joint, which is a synovial joint.
The knee synovial joint is mainly filled with types of compounds, hyaluronan, and aggrecan, with some Collagen added in. We know that taking supplements of Glucosamine Sulfate around 1500 mg does seem to make the knees feel better.
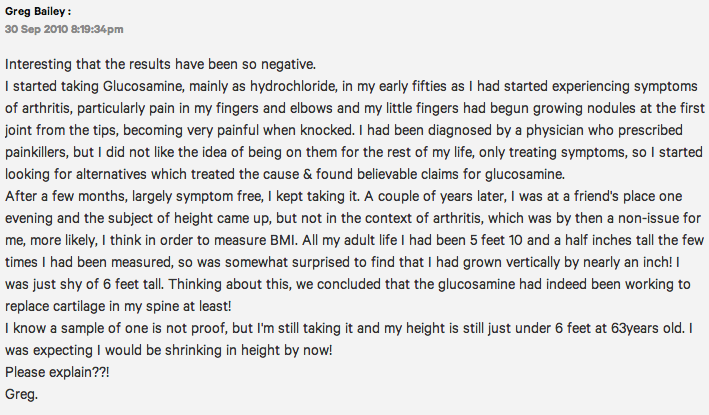
T he cheapest way to possibly grease up the surface of the articular cartilage would be to take those glucosamin sulfate at 1500 mg twice a day, for upwards of 3 months. The added collagenous material could possibly cause the cartilage to get slightly thicker. From This Link Here, a guy named Greg Bailey from Australia back in Sept 2010 stated that he grew from 5′ 10″ all of his adult life to almost 6 feet tall in his 50s from taking Glucosamine. See the picture to the right…
he cheapest way to possibly grease up the surface of the articular cartilage would be to take those glucosamin sulfate at 1500 mg twice a day, for upwards of 3 months. The added collagenous material could possibly cause the cartilage to get slightly thicker. From This Link Here, a guy named Greg Bailey from Australia back in Sept 2010 stated that he grew from 5′ 10″ all of his adult life to almost 6 feet tall in his 50s from taking Glucosamine. See the picture to the right…
This is not the only case where ingesting Glucosamine Sulphate seemed to make people grow taller. There is a very famous article written by a person named Jennifer Hope (Hope???) entitled “Can a pill make you taller in four weeks?” which also stated that taking Glucosamine Sulfate at 1500 mg daily for around 1 month will make you around 2-4 mm taller.
 Price: $22
Price: $22
Directions: Take 2 of the tablets, which combine for a total of 3000 mg of Glucosamine Sulfate every day, 1 during the morning and 1 during the evening.
I am part of the Amazon Affiliate program so if you buy it from the link above I do get a small bit of commission earnings. (which is around $1 for each bottle you buy)
Or you can buy the Glucosamine Sulfate at 1500 mg and just take 1 pill a day…
 Price: $39 w/ Free Shipping
Price: $39 w/ Free Shipping
So if the ingestion of the Glucosamine is something one does not want to try, there is something slightly more invasive which I propose at this point which probably has a high chance of getting through.
However a much more effective way is to get a syringe and use the StemPro® Chondrogenesis Differentiation Kit sold by Life Technologies. You want to combine the StemPro Chondrogenesis Differentiation Kit with the BMP-7 sold by Life Technologies as well. In my previous posts comparing the dozens of current growth factors out there which are most effective in getting the progenitor cells to differentiate into the chondrogenic line, BMP-7 aka OP-1 is the most chondrogenic, compared to say BMP-2, BMP-6, or BMP-9.
You want to get the angle just right to get the initial syringe just along the surface of the middle of the articular cartilage of the proximal tibial epiphysis. The first injection will be the right mesenchyme, the MSCs, and the 2nd injection, using the same needle as a vessel would be the administration of the BMP-7, to get the progenitor cells to differentiate into the chondrocytes, which will over time diffuse downwards the articular cartilage into columns. To activate the chondrocytes to hypertrophize, you can use the various methods of chondrocyte hypertrophy that Tyler has talked about over the years, which range in a variety of subjects.
Note: If you take the 2nd approach, it might be slightly hard to obtain these tissue engineering lab components. That will be the 1st major hurdle since this type of material seems to be available only for medical professionals, physicians and researchers. Of course, I am aware that there is at least 1 person who regularly reads this blog who just finished their medical school and was doing their first year residency.
Note #2: You want to also get a biopsy of your cartilage tissue and issue how your own immune system it will react to the injected MSCs and BMP-7. BMP-7 which is just a growth factor by itself should be the same in all humans so the human body’s immune system should not react when it gets injected, but the MSCs might be. When doing an ear or nose piercing for a new stud or earring, it might be smart to save the fibrocartilage material and test how the cartilage tissue in calf serum medium would react with the MSCs injected into it. It is also suggest that a 2nd biopsy is done with some extracted blood and have a histological examination to see how your bodies immune system will react to the injected MSCs. Will it start to go into inflammation, White T-Cells attacking it, Red Platelets clogging around it, or maybe nothing at all?
So to do the 2nd part, for safety reasons, you will be required to do an immunological testing to see whether the MSCs you did get will be okay with the overall system. I would guess that if one did manage to get the cells and the growth factors on the top of the articular cartilage, the result would be upwards of just 1 cm in increased height, if there is adequate induced chondrocytes and the right technique for chondrocyte hypertrophy is chosen.
Tyler’s Notes:
It has been established that longitudinal bone growth occurs at the articular cartilage of some bones as shown by some finger studies. However, the joint and epiphysis may constrain this growth. Possibly related to the periosteum. Endochondral ossification has been shown to occur at many joint areas.
Longitudinal bone growth is not significant in the articular cartilage due to some constraint from the epiphysis or the joint. There have been studies showing that the periosteum constrains growth and that periosteal stripping can enhance growth. Since LSJL is applied on the joint cavity it could influence the mechanisms by which the joint cavity and epiphysis constrain growth. However, LSJL seemed to upregulate periosteal related genes. But none of the genes were periosteum specific so it could’ve just been a correlational effect. And the afformentioned study, compared the perichondrium to the periosteum rather than the periosteum to the bone. If the perichondrium does not constrain growth whereas the periosteum does it’s possible that the LSJL could enhance growth by altering the shape of the periosteum so it is not so growth constraining. LSJL did upregulate perichondrium genes much more than periosteum genes.
I’d like to also mention a note from the study “Metacarpophalangeal length changes in humans during adulthood: A longitudinal study” which states “When cartilage thickness exceeds the critical dimensions that limit nutrition by diffusion, the cartilage cells hypertrophy and degenerate, the spaces become vascularized, and osteoblasts develop to initiate endochondral bone formation in the midst of the articular cartilage.”<-So a primary way to induce endochondral ossification is to just increase articular cartilage thickness.
Conclusion:
1. Articular cartilage undergoes endochondral ossification.
2. This endochondral ossification results in longitudinal bone growth in bones that do not have joints or epiphysis such as the bones in the fingers.
3. Identifying what in the joint or epiphysis constrains growth and how to disrupt this may allow articular cartilage to generate longitudinal bone growth in long bones with a joint and epiphysis. Although as shown in the finger studies, growth via articular cartilage is very slow.