Go to this page to see the original x-rays. Here’s a picture that shows that my right finger is longer than my left. However, what’s interesting is that the phalanx bones of the left index finger are actually longer than the right index finger. So, I turned to the metacarpal bone of the index fingers and it turns out that the right metacarpal of the index finger is longer than the left and a longer metacarpal would explain the increased finger length in the image in the second link below.
LSJL may have lengthened all the bones of my right finger but because my left finger was always longer it may have only reduced the discrepancy. If every single bone on the left side of body is longer than the right except for those that I performed LSJL on I submit that as proof of LSJL. A possible reason that all my left bones are longer than my right bones but all my right bones are thicker could be related to FGFR3 and CNP. My left side could have had less of the FGFR3 receptors or more of the CNP receptors.
I didn’t know that all my left sided bones were longer than my right until recently. I just assumed it was due to my scoliosis or it was just an illusion because my right side was thicker. So unfortunately, I did not account for it when designing to the experiment. But again, if every single bone on my hands is longer on my left than my right metacarpal which is where I performed LSJL then we can take that as evidence that LSJL works.
Here’s a video with my right finger before any loading.:
Here’s the left hand before video:
My right index finger metacarpal did grow longer but it would appear that my other bones did not. I say appear because it turns out that all my bones on the left side of my body are longer than the left. Thus, any growth may actually just be shown by decreasing the gap between the right and left finger bones. The right finger bones may have grown but that would not show up because the left finger bones were still longer. If every single bone has the version on the left side be longer, but the one bone that had LSJL on it can we say that LSJL induced growth?
Here are the metacarpals of my right and left index fingers:
The lines are very straight. I got pretty close to measuring out straight lines. I measured the right metacarpal as being 1383.0 pixels long. I got 1372.0 pixels long for the left metacarpal. The left metacarpal might extend a little below the line but I zoomed in so I could get things accurate. Right metacarpal is 0.8% longer. Now here’s thing about the right finger being 0.8% longer. All my left bones in my body are longer than the right bones but the right bones are thicker. Thus, the right metacarpal may have grown to catch up to the left metacarpal and then grown further. So actual growth may be larger than that.
I performed LSJL only on my right finger. Here’s an analysis of the other bones of the index finger:
The slope of the line may be off by about 0.11 degrees or so which is very minor. The left finger actually measures out longer.
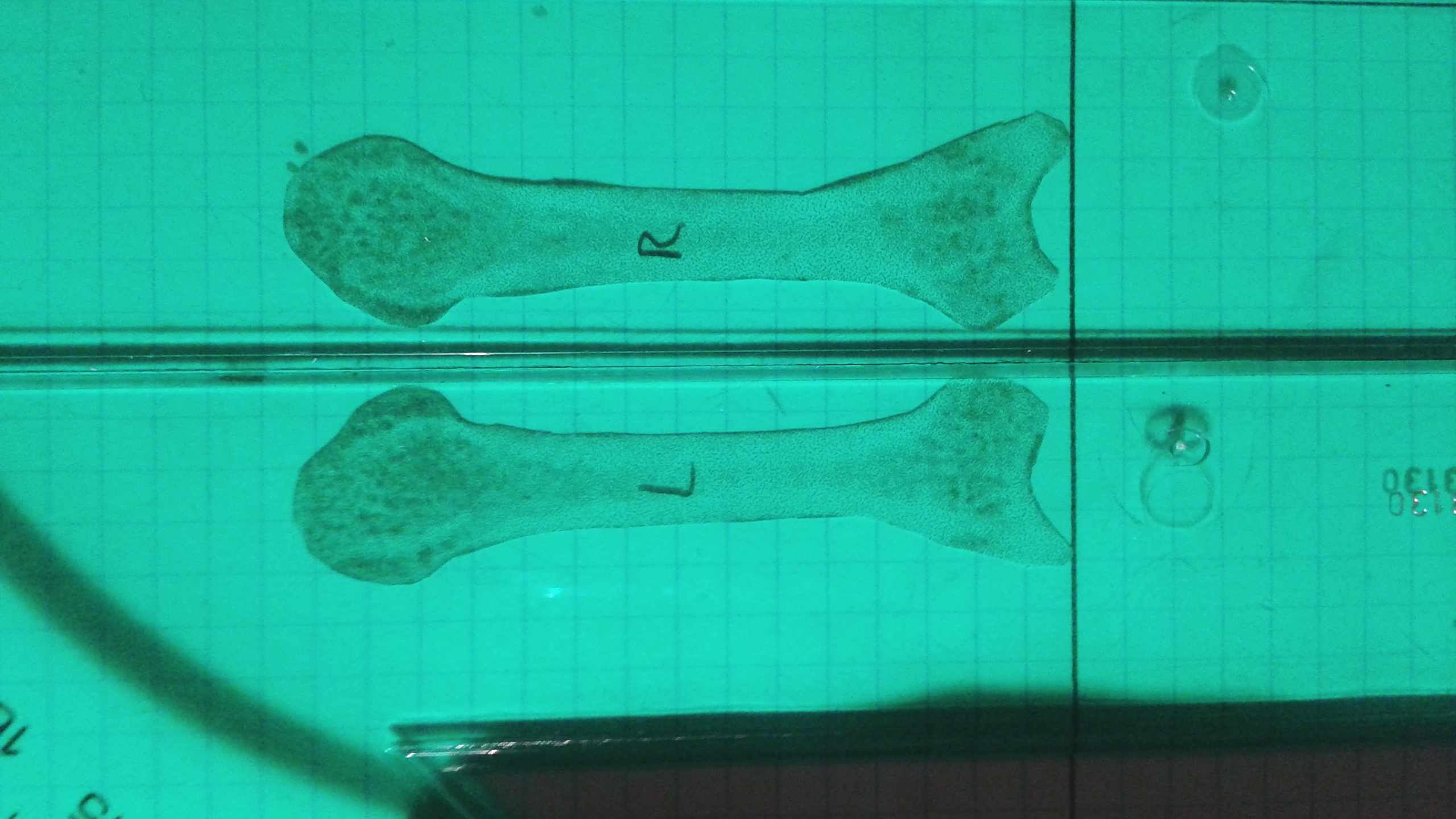
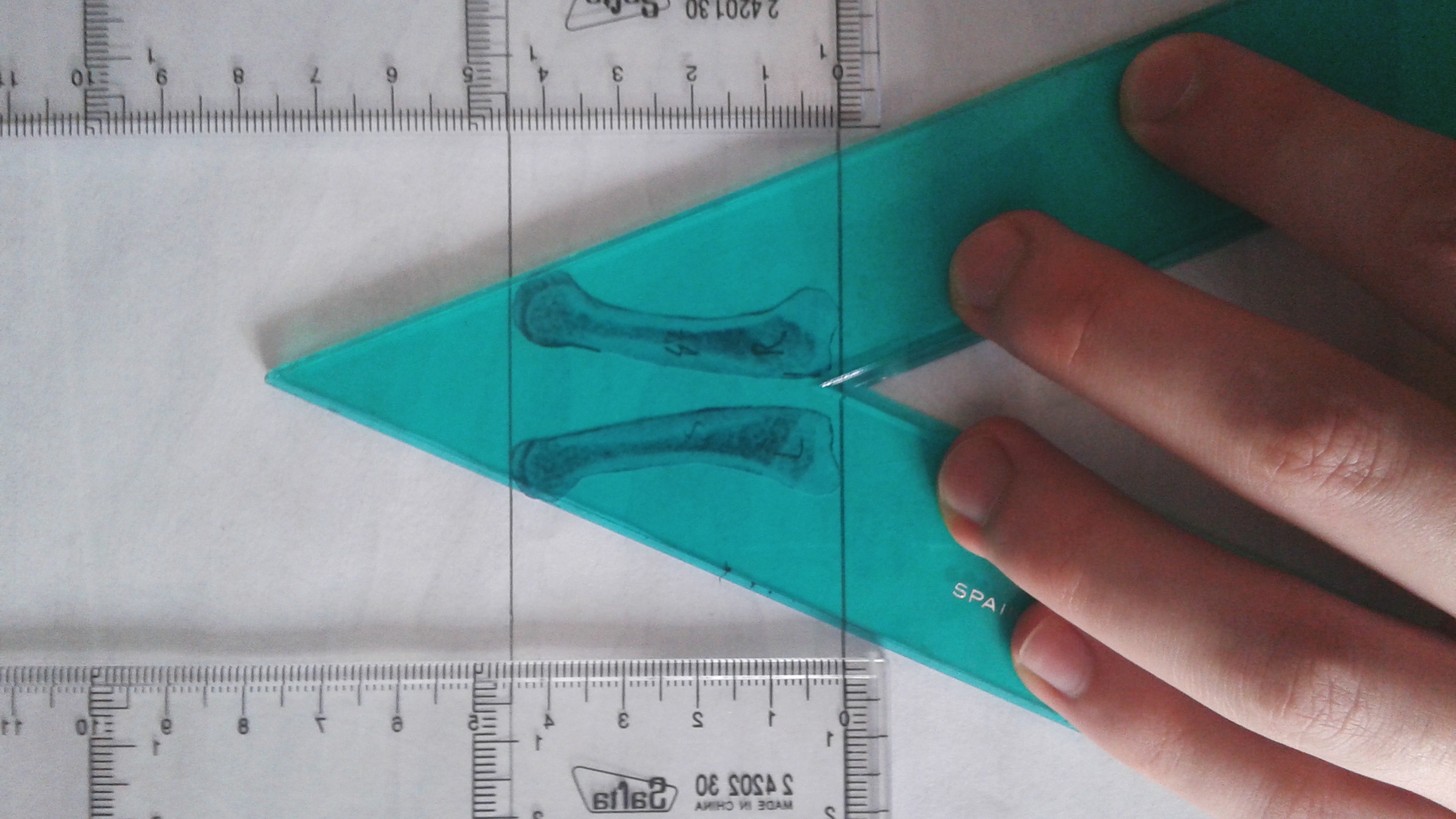
Here’s an image of my proximal index fingers: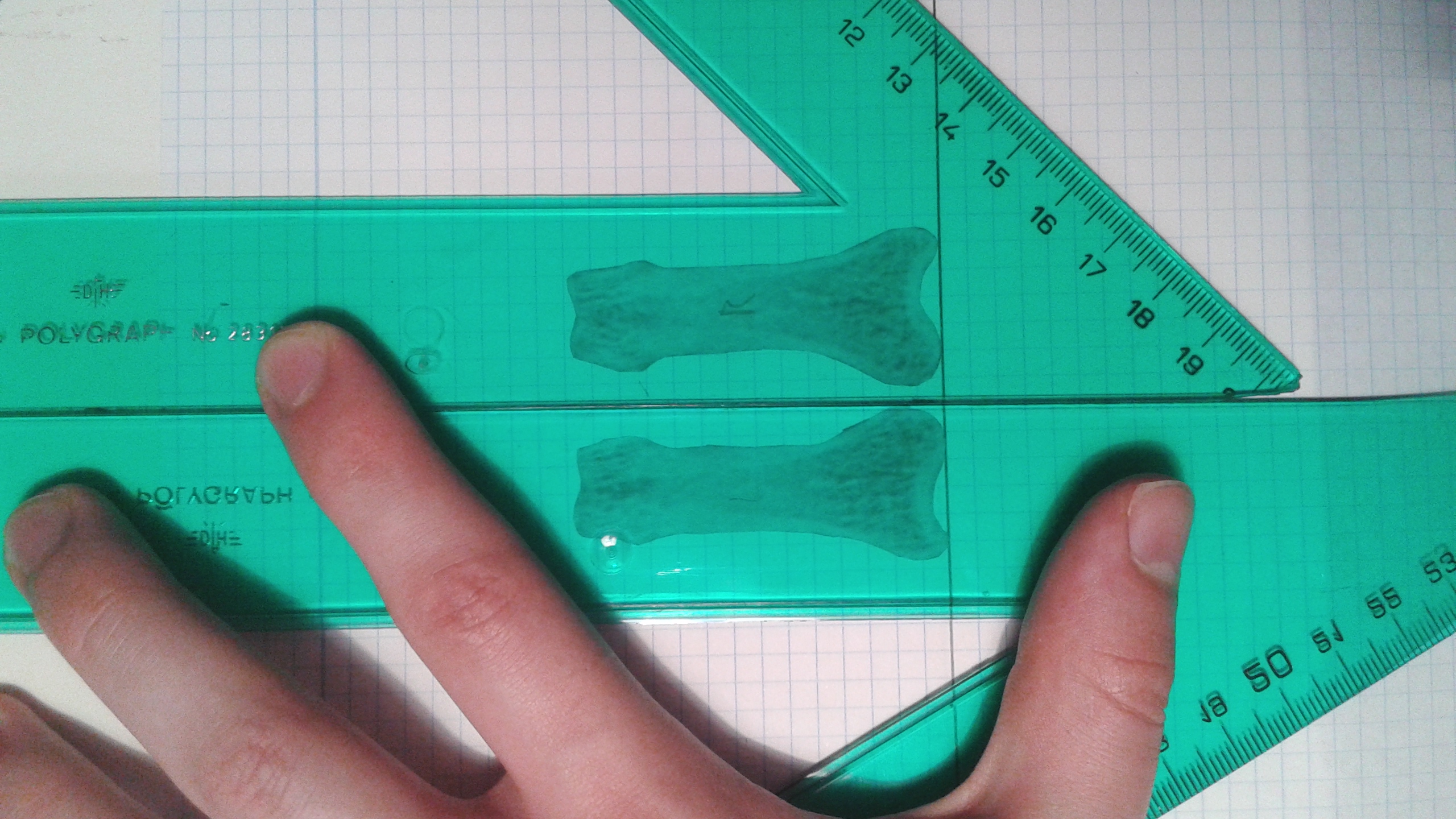 This is a cut out of the proximal index fingers of the right and left finger bones from the x-ray from the link provided above. Click on the image as the image shows flipped for some reason. The right bone is the one labeled with the R. The measurements were done by adjusting the two bones until they were as long as possible. This insures that both bones were given the same advantages and the angle at which I put my finger is not a factor. Measurements were done by someone else.
This is a cut out of the proximal index fingers of the right and left finger bones from the x-ray from the link provided above. Click on the image as the image shows flipped for some reason. The right bone is the one labeled with the R. The measurements were done by adjusting the two bones until they were as long as possible. This insures that both bones were given the same advantages and the angle at which I put my finger is not a factor. Measurements were done by someone else.
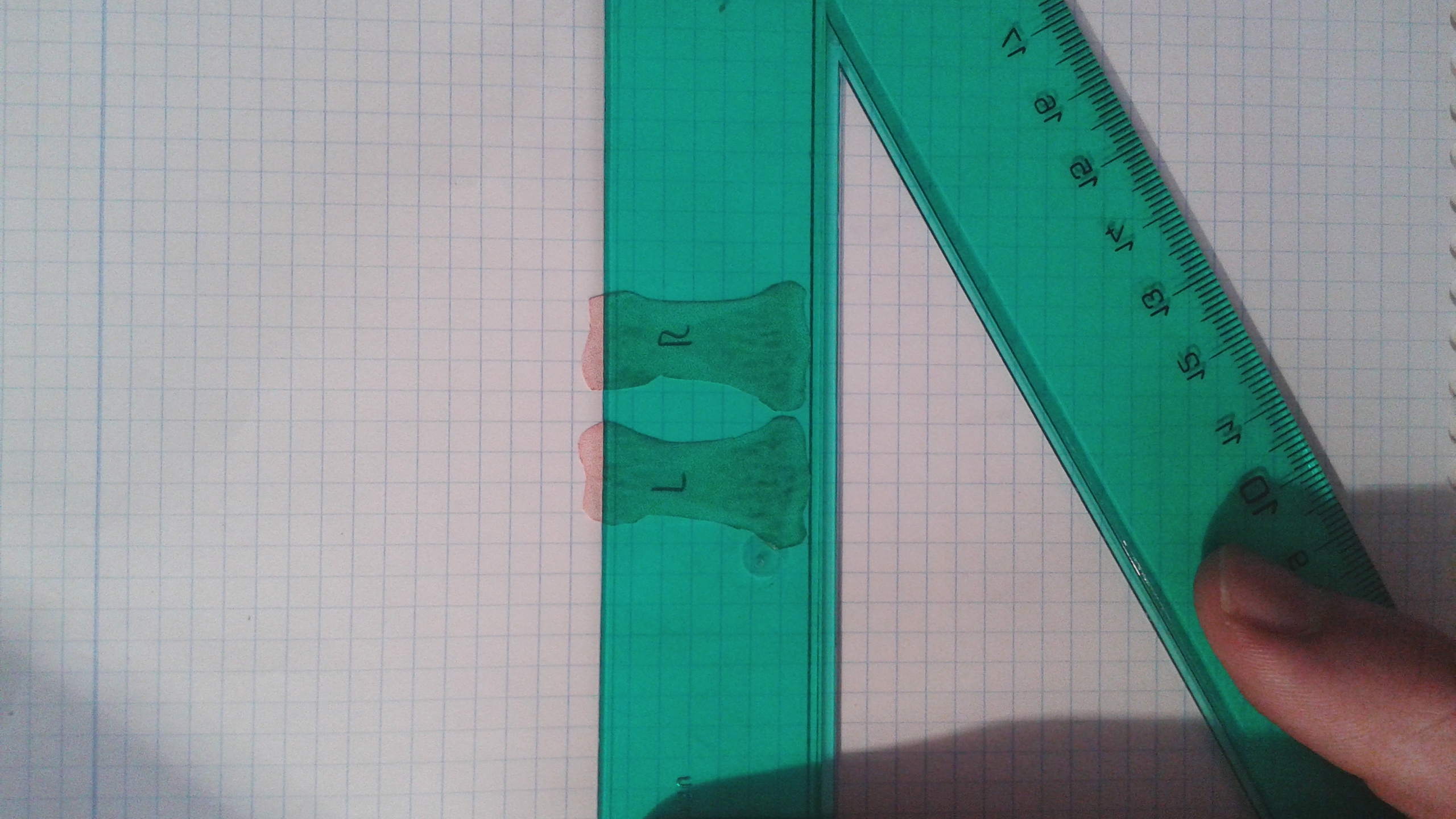
The lines on the graph are slightly off the vertical lines sloping down at a 1.2 degree angle towards the right side of the computer screen(using the image if you click on the image not the inverted one here). This images slope favors the right side so the right side will appear longer if you don’t correct for the one degree.
Here’s another image:
 This one slopes to the right only at about .80 degrees(measuring the straight line downwards it is .80 off from 90 degrees. This images slope favors the right as well but not nearly as much. The left bone is longer.
This one slopes to the right only at about .80 degrees(measuring the straight line downwards it is .80 off from 90 degrees. This images slope favors the right as well but not nearly as much. The left bone is longer.
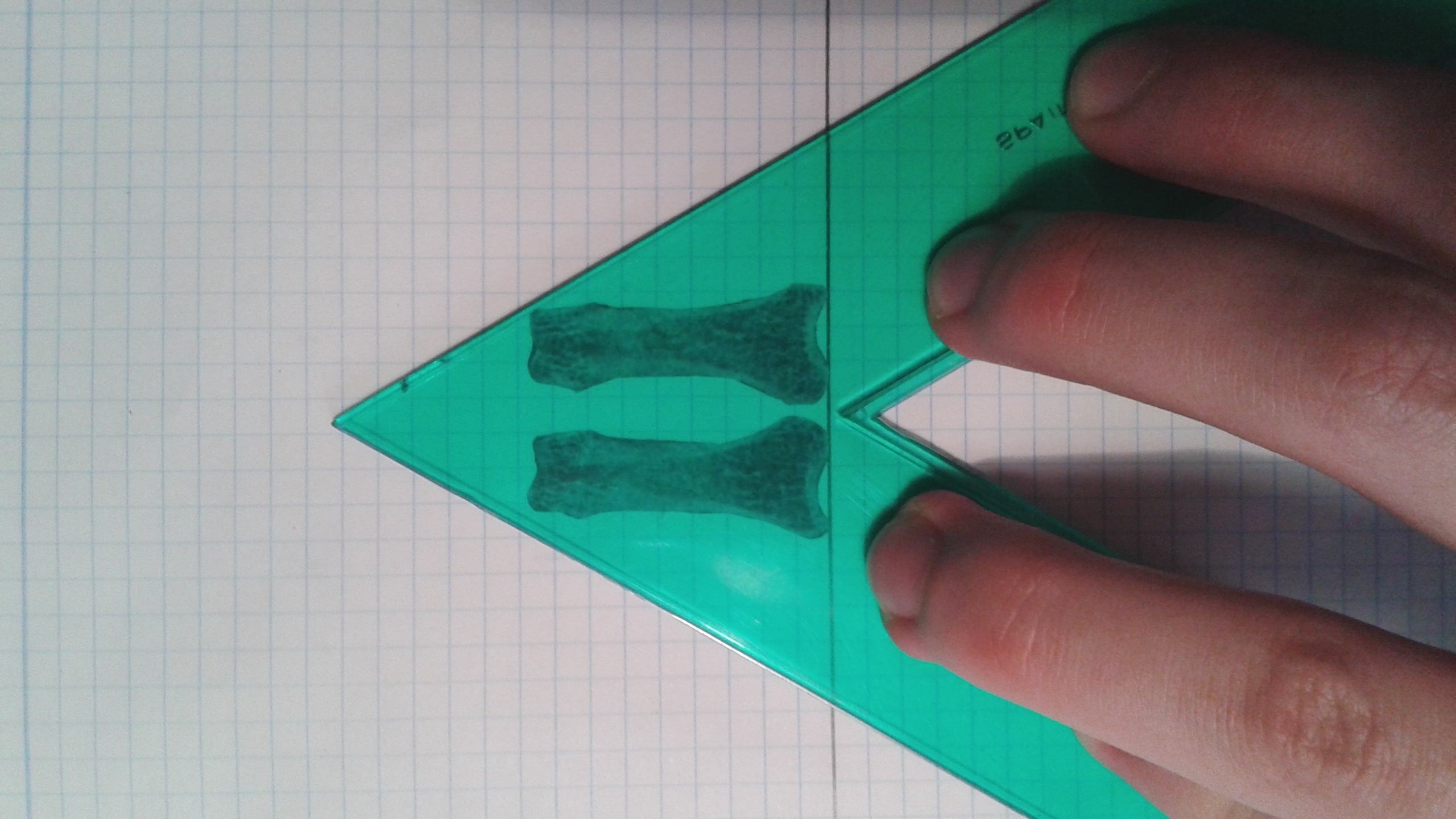
Here’s the cutout of the lateral view:
 You can see here the the epiphysis of the right index finger are much larger but the left finger is longer overall.
You can see here the the epiphysis of the right index finger are much larger but the left finger is longer overall.
How I’m changing my performance of LSJL now:
Next step is to confirm that all my left handed bones are longer except for that metacarpal.
Now since I have the x-rays, I’m going to be performing LSJL on both my right and left index finger. Since I have x-ray images, I have those as a control using one of the fingers as a contralateral control is less important.
Previously, I was limiting my clamping based on my left side since my right side is stronger and thicker but since my left side is longer I’m not going to be clamping with whatever I can handle safely for my right side and whatever I can handle safely with the left side and not worrying about clamping them with the same intensity or amount of time. Since my right side is so much stronger it should be able to withstand more clamping. Thus, it was my goal with this to correct for the discrepancy between the right and left side in addition to increasing bone length overall.