What I Learned From Attending The Annual 3D Printer World Expo
 Since the annual 3D Printer World Expo was being held this year at Seattle, (more specifically Bellevue, WA) I bought tickets to attend the expo and listen to the speakers talk about the revolution that is taking place right at this time, which will revolutionize the world in the coming decades to come.
Since the annual 3D Printer World Expo was being held this year at Seattle, (more specifically Bellevue, WA) I bought tickets to attend the expo and listen to the speakers talk about the revolution that is taking place right at this time, which will revolutionize the world in the coming decades to come.
The event was being held from August 22-23, 2014 which concluded tonight. I decided only to attend the conference the first day, and talk with all of the people at the exhibits to see how far they have come along in being able to develop products for medical application.
There was three main reasons why I decided to attend.
First, I realize that the revolution of 3D Printers is going to bring about a paradigm shift in the form of a disruptive technology, similar to how the company Uber is trying to transform the taxi service industry. It is absolutely critical to keep up with the real edge of what is going on in the world today. At the expo, I was able to try out the Oculus Rift that people in the tech world have all been going crazy for, with the people from Prizmiq.
Second, I wanted to see who is already trying to create biocompatible implantable hyaline cartilage, by combining the fields of tissue engineering and stem cells, for what I believe will be the real revolution for our endeavor.
Third, I have started to go into research on the developing technology of turning humans into androids/cyborgs. I have already jumped on the BioHacking bandwagon, promoting the idea set forth by David Asprey, but I feel like there is much further we can go to integrate the electronic world with the biological world.
I took pictures, got free stuff, and talked to people who are in the industry who are promoting their businesses and products.
For our purposes though, I asked each of companies that was selling or promoting 3D Printers the question, “Are you guys selling 3D Printers that has the ability to print bio-compatible, in vivo implantable functional human cartilage?”
Almost all of the companies I talked to said no, except maybe 1 company (Nytec). When I asked just how fine the filaments threads can get to in terms of accuracy in making these 3D Models, the smallest I found was around 7-8 microns, with the upper end being around 200 microns.
Here is some things which they did tell me which is being created.
PEEK BIo-Material (poly-ether-ether-ketone) – Unlike the PLA and the ABS type plastic extruded filament material that is traditionally used to make 3D models, there is a another material that is coming out known as PEEK Material. It has been used apparently for the last decade and has slowly had multiple variations/derivatives of the PEEK material made. Its various materials characteristics makes it the most attractive material to be used for in vivo implants. (Refer to study “PEEK Biomaterials in Trauma, Orthopedic, and Spinal Implants” or “In vivo biocompatibility testing of peek polymer for a spinal implant system: A study in rabbits“)
Organovo – This company I have done research before, and it seems like they are the main company to focus on. The people who organized the 3D World Expo when I asked them specifically named this company for 3D Printing Implantable Tissues. I originally referred to Organovo when I wrote about the possibility of using the biomedical practice of Bioprinting aka Electrospinning in the post “Increase Height And Grow Taller Through Bioprinting And Electrospinning“. On the company website, they state the following…
“…Our 3D bioprinted human tissues are constructed with precision from tiny building blocks made of living human cells, using a process that translates tissue-specific geometries and cellular components into 3D designs that can be executed by an Organovo NovoGen Bioprinter. Once built, the bioprinted tissues share many key features with native tissue, including tissue-like cellular density, presence of multiple cell types, and the development of key architectural and functional features associated with the target native tissue.”
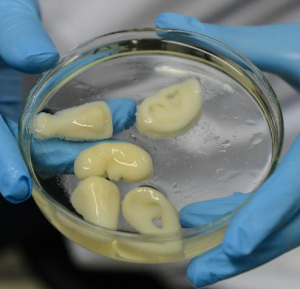 Regenovo – This seems to to be China’s answer to Organovo. From the 3DPrintersIndustry.com website, they say that the China based Regenovo is still about 15 years away from being available to the average patient. It is a type of”…medical grade 3D bioprinters that is still under development and showing promising results“. The researchers at Regenovo have already been able to bioprint out a fibrocartilage based ear type tissue, as well as potentially also noses.
Regenovo – This seems to to be China’s answer to Organovo. From the 3DPrintersIndustry.com website, they say that the China based Regenovo is still about 15 years away from being available to the average patient. It is a type of”…medical grade 3D bioprinters that is still under development and showing promising results“. The researchers at Regenovo have already been able to bioprint out a fibrocartilage based ear type tissue, as well as potentially also noses.
Since Regenovo is already able to print out nose and ear structures in about 1 hour!!, they should be able to re-create the chondrocyte column like structure that is found in the epiphyseal hyaline cartilage which can be a mass-produced synthetic growth plate which can be popped into a bone resection to lengthen the bone. The researchers are from some university in Hangzhou and are working with Independent Intellectual Property Rights (IIPRs). The developer named Xu Ming-en is able to create a 4-5 inch wide ear cartilage part within 1 hour already using the regenovo 3d bioprinter.
From the website 3DPrinterWorld.com website, what we are seeing is that along with Organovo & Regenovo, there are labs in Universities around the world like Wake Forest, Cornell, and the University of Iowa who are all working on very similar areas of focus, aka cartilage and spinal disc regeneration.
Taulman3D.com – This company supposedly got a FDA approval also a day ago for using their implantable nylon based material for medical applications.
Selective Laser Sintering (aka SLS) – This is a type of way of 3D Printing method based on using a laser to add more material on the object you are trying to shape and form. Currently, I know very little about this type of manufacturing technique, although it seems to be one of the manufacturing industries most common approaches to making parts.
One company I talked to say that SLS might be able to be used to make implantable parts. I forgot which one though by now.
However, what I have noticed is that due to the nature of the filament (aka raw materials) you are heating up and extruding through the extruder head, these materials like the most two types of filament material, PLA and ABS just can’t be used for medical application, since they would poison the person who tried to put the thermoplastic either in their body or on their skin. Now, there are many, MANY, companies right now who are using 3D Printers to build and make prosthetics, (like for instance Coyote Design & Mfg based in Idaho) by making bone like-tissue which will be placed along the skin but very few companies have been able to succeed in printing things that would work okay inside the human body.
Here is something I didn’t realize maybe months ago when I was writing about the possibility of using 3D Printers to print out our own internal organs. Currently, there is maybe about just 2 dozen types of materials that you can use as the raw material in the filament to make the models and shapes that you want. Here are some of the most common types…
- ABS
- HIPS
- PLA
- NYLON
- PVA
- TPE
- T-GLASE
What to take away from it all…
I have been trying to combine all of the areas/fields that I am interested in and doing research on into one. So far, that has led me into the field of 3D Printers and finding the right type of collagen/scaffold configuration to create new cartilage tissue.
It has already been shown by at least 2 sources that making a 10 cm wide piece of fibrocartilage layer is already possible, taking just around 1 hour. I am wondering just how hard would it be to turn that ear/nose piece already made in multiple university labs around the world into hyaline cartilage and make the type of functional implantable cartilage that can expand and make our bones grow volumetrically. Not too hard I suppose.
If the researchers really wanted to, they would be able to get the new growth implant implantations available for the general public’s use within maybe just 3-5 years if they actually put all their effort and focus into it.
To end this post, I give you a vision of what will almost definitely come about in the future, with the forward being presented by former Lucasian Professor of Cambridge, Dr. Stephen Hawking, on how medical breakthroughs have allowed him to live and function beyond the years expected of him when he was first diagnosed with Lou Gehrig’s Disease decades ago.

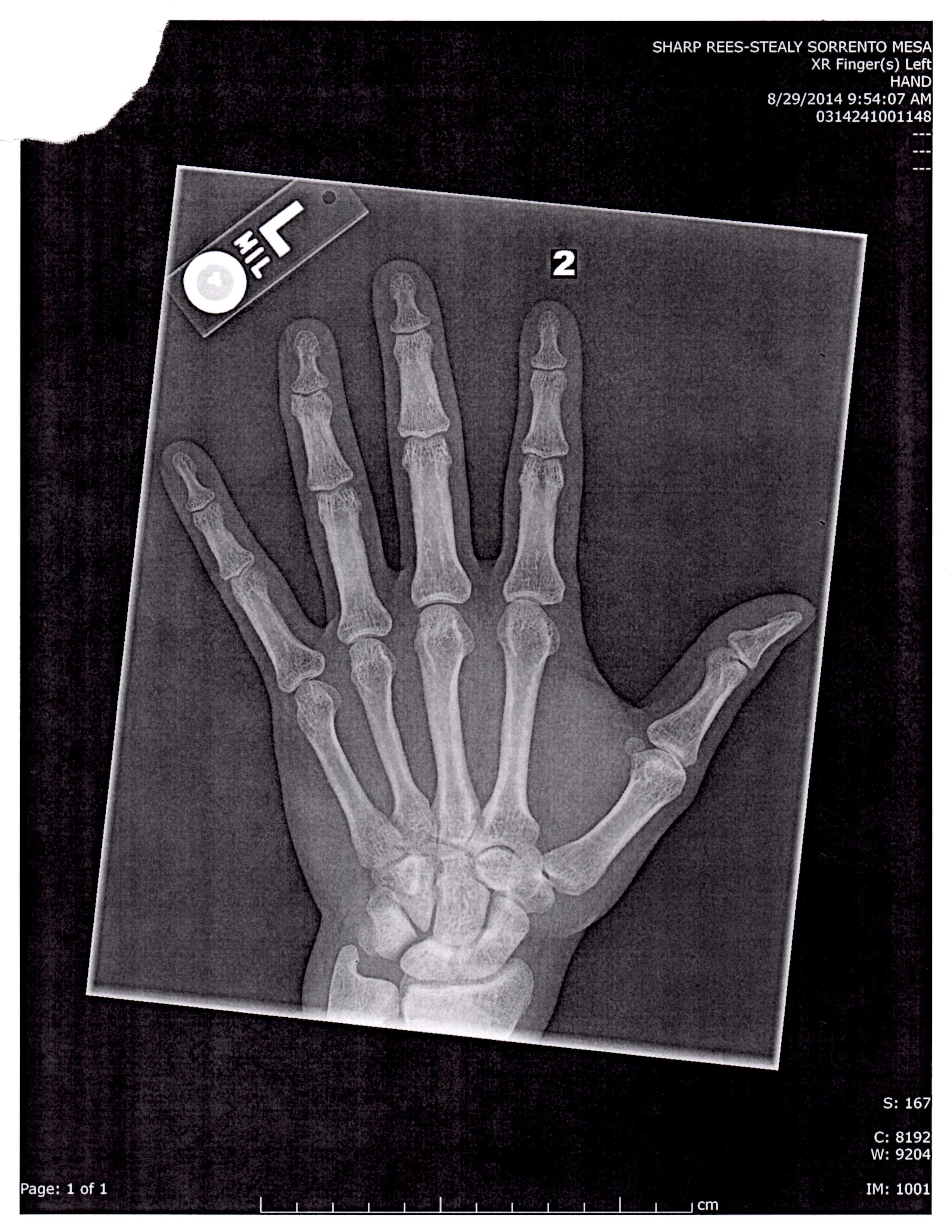
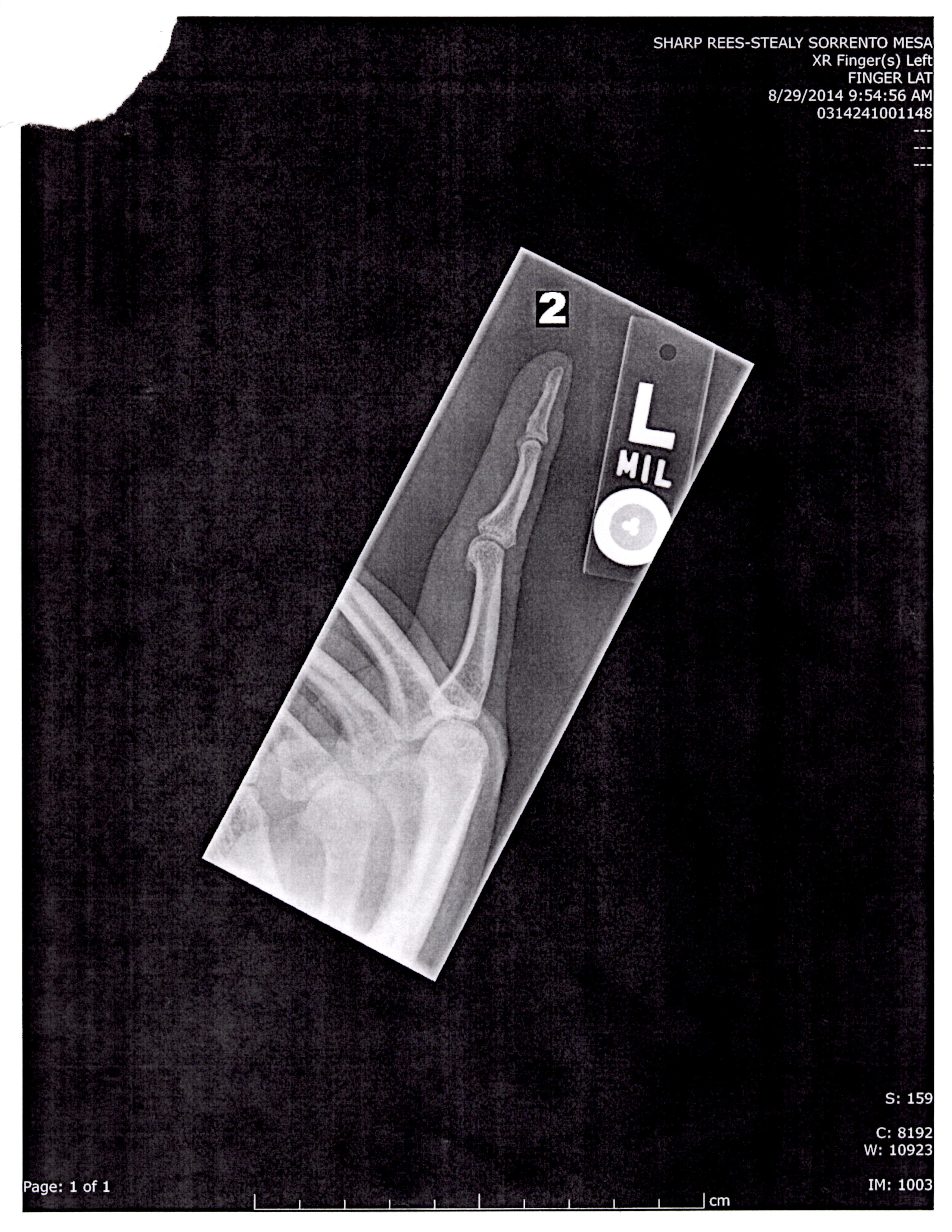
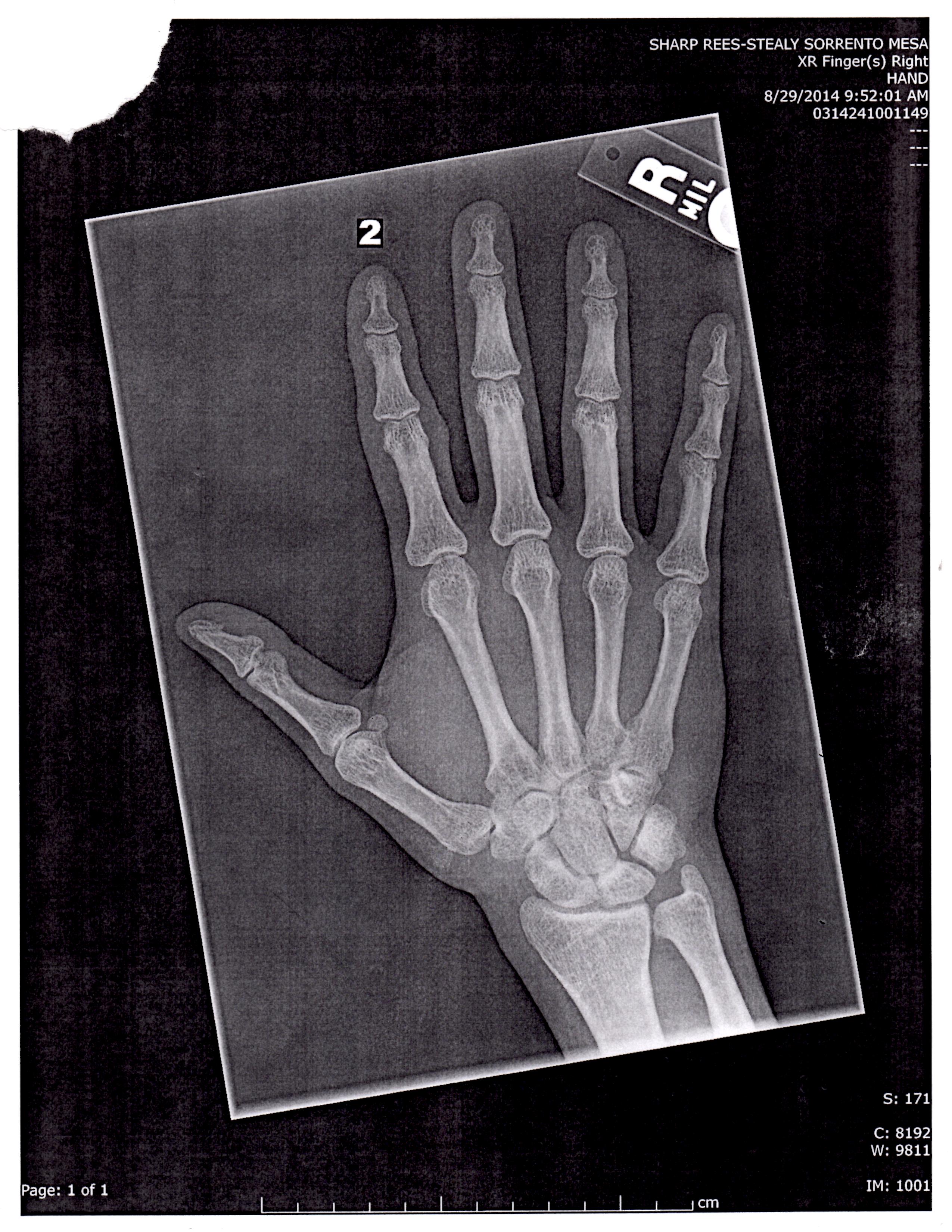
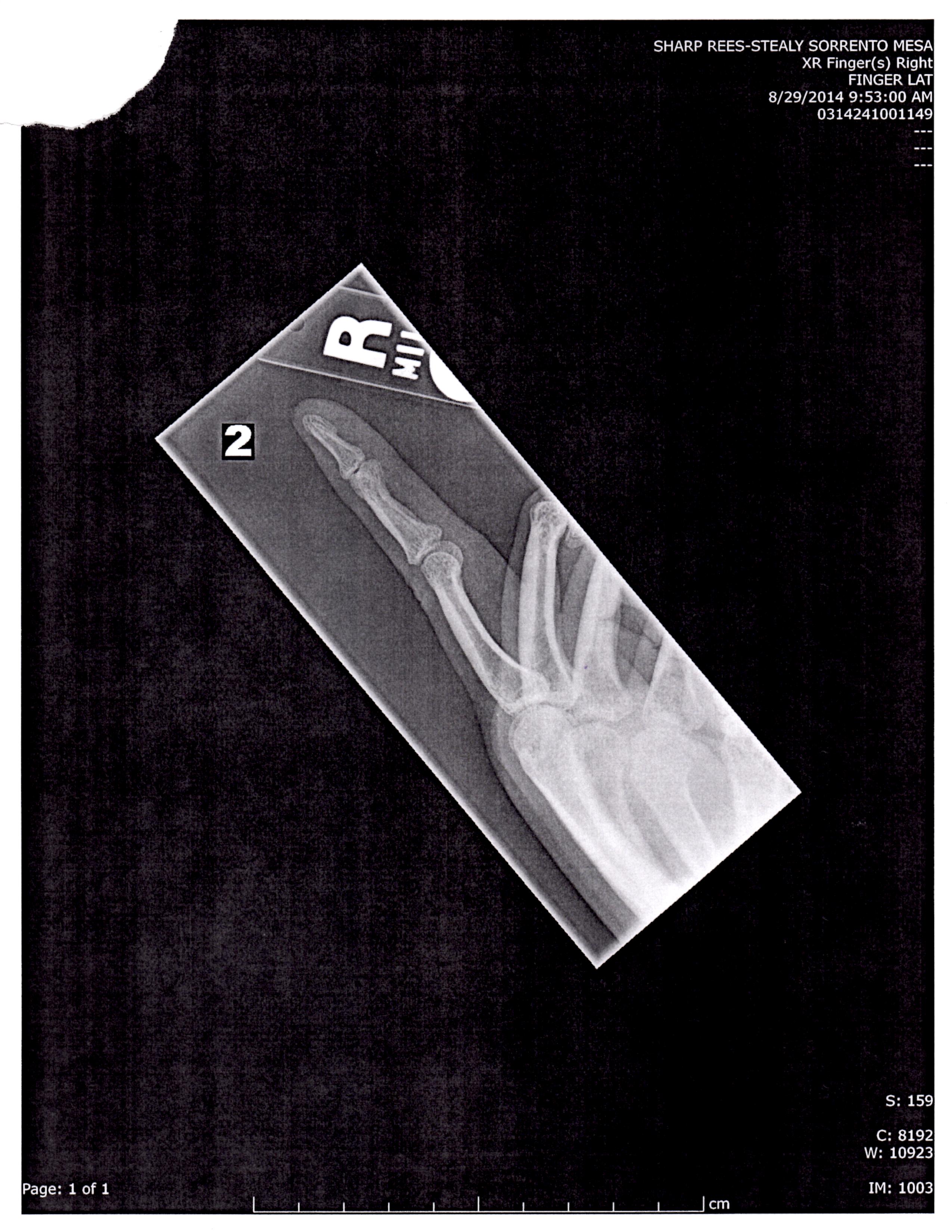
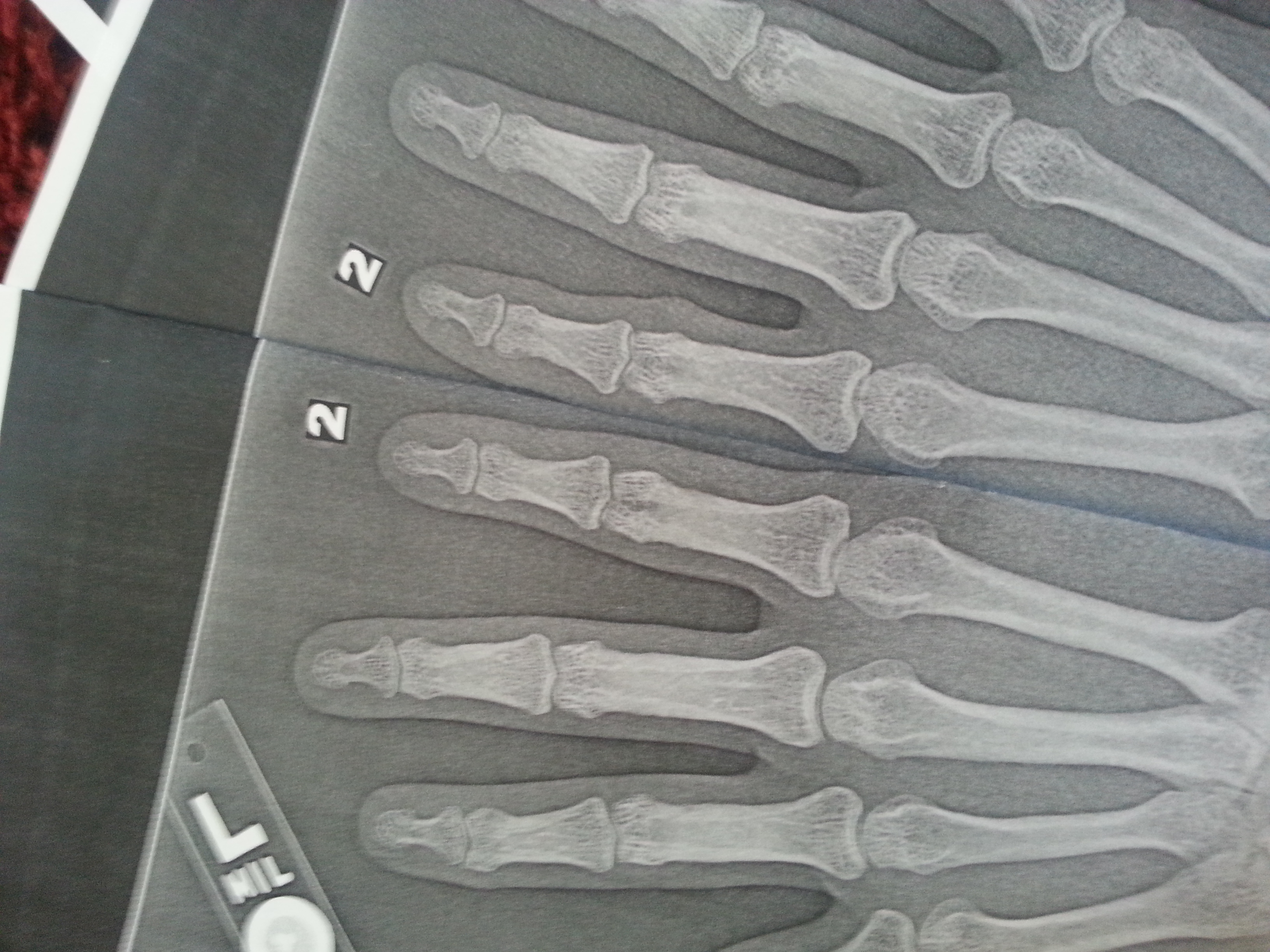 The right index finger is longer than the left although I will have to do further analysis with GIMP or have Michael or someone do independent analysis. Same with the left thumb(clamped thumb being longer than the right).
The right index finger is longer than the left although I will have to do further analysis with GIMP or have Michael or someone do independent analysis. Same with the left thumb(clamped thumb being longer than the right). The lump is completely in the soft tissue and cannot contribute to height (see the x-rays)
The lump is completely in the soft tissue and cannot contribute to height (see the x-rays)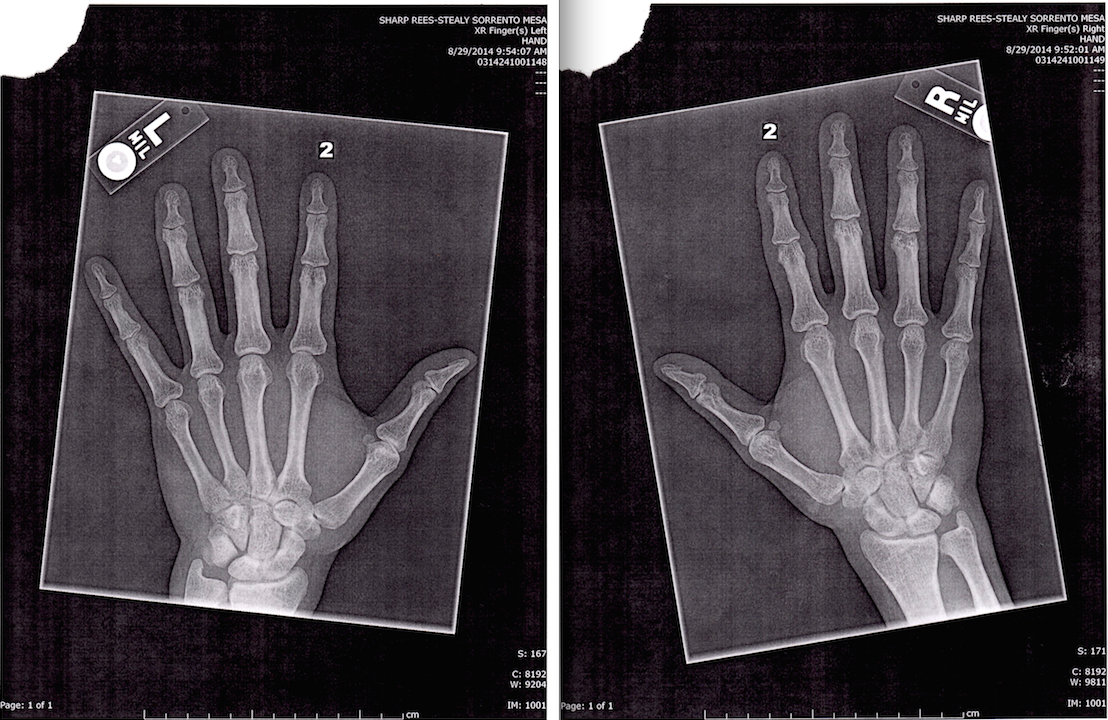


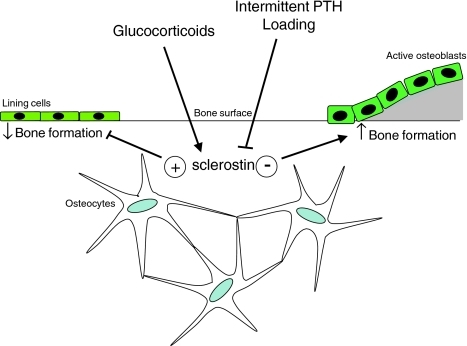
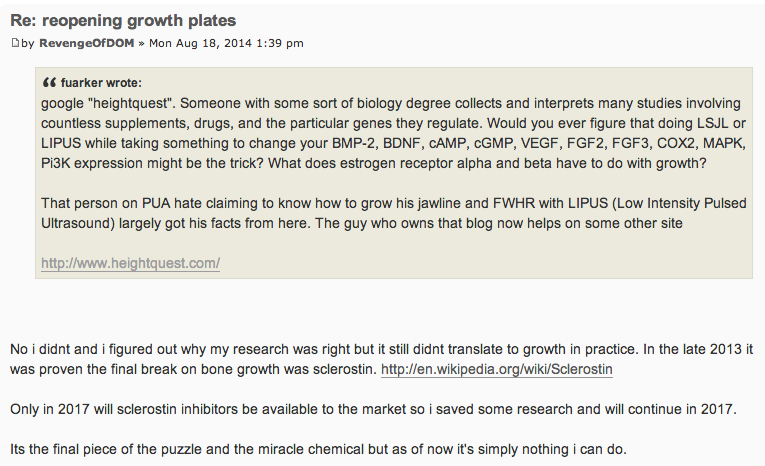 It seems that this guy has also been doing his own research on growing taller like us in parallel. It is just that he does not publically publish what he finds. His mention of the class of chemicals which can inhibit this compound known as Sclerostin shows that he understands the stuff very well.
It seems that this guy has also been doing his own research on growing taller like us in parallel. It is just that he does not publically publish what he finds. His mention of the class of chemicals which can inhibit this compound known as Sclerostin shows that he understands the stuff very well.