Knowing that H blood vessels are lost via aging is a breakthrough as it may indicate that restoring type H blood vessels may be key to restoring the growth plate.
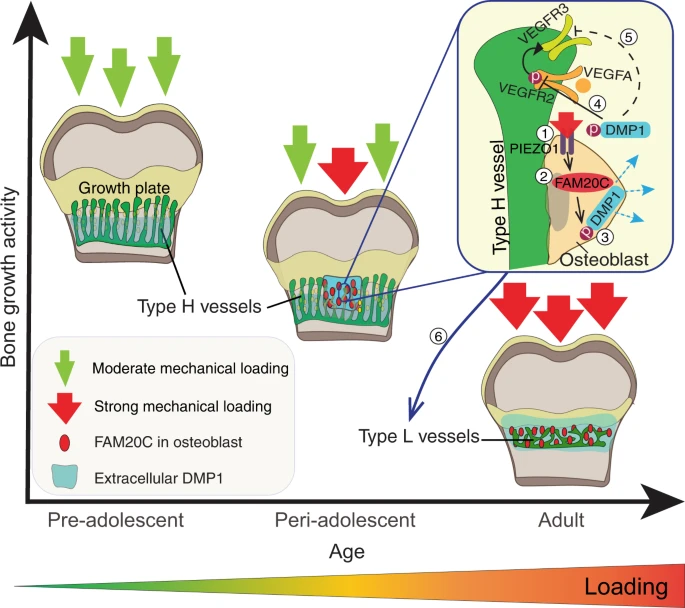
“Bone growth requires a specialised, highly angiogenic blood vessel subtype, so-called type H vessels, which pave the way for osteoblasts surrounding these vessels. At the end of adolescence, type H vessels differentiate into quiescent type L endothelium lacking the capacity to promote bone growth.{How do we reverse this process?} Until now, the signals that switch off type H vessel identity and thus limit adolescent bone growth have remained ill defined. Here we show that mechanical forces, associated with increased body weight at the end of adolescence, trigger the mechanoreceptor PIEZO1 and thereby mediate enhanced production of the kinase FAM20C in osteoblasts.{so if we are underweight type H blood vessels will stay around longer?} FAM20C, the major kinase of the secreted phosphoproteome, phosphorylates dentin matrix protein 1, previously identified as a key factor in bone mineralization. Thereupon, dentin matrix protein 1 is secreted from osteoblasts in a burst-like manner. Extracellular dentin matrix protein 1 inhibits vascular endothelial growth factor signalling by preventing phosphorylation of vascular endothelial growth factor receptor 2. Hence, secreted dentin matrix protein 1 transforms type H vessels into type L to limit bone growth activity and enhance bone mineralization.{so a dentin matrix protein 1 inhibitor may be a possible mechanism in which to grow taller?} The discovered mechanism may suggest new options for the treatment of diseases characterised by aberrant activity of bone and vessels such as osteoarthritis, osteoporosis and osteosarcoma.”
” Type H vessels are located exclusively at the sites of active bone growth, namely the ossification front (OF) and periosteum, and they are organised in columnar structure. Notch signalling, Hypoxia-inducible factor 1-alpha (HIF1α) activity, blood flow speed and slit guidance ligand 3 (SLIT3) were shown to support type H vessel formation”
“endothelial cells in bone require integrins for their proper functioning and maintenance, which highlights extracellular matrix (ECM) proteins as important factors for endothelium activity”
” we performed laser microdissection (LMD) of single capillary with associated surrounding cells in the OF of juvenile (4-week-old) and adult (12-week-old) mice.”
“Our detailed analysis of DMP1 protein localisation throughout postnatal bone development showed that until 5 weeks of age, the protein was mainly localised at the base of the zone of type H vessels in the [Ossification front]”
“DMP1 accumulation in the OF[Ossification Front] centre at 5.5–6 weeks correlated with a decrease in endomucin (EMCN) intensity and reduced amounts of MMP9 at the OF-GP border. This was associated with the disappearance of bulges and columnar structure of the vessels”
They found though that the DMP1 knockout femurs were shorter at a certain age point but perhaps a reduction in DMP1 would lead to slower more sustained growth.
“DMP1 secretion correlates positively with body weight and coincides spatiotemporally with FAM20C upregulation”
“mechanical loading through increasing body weight or/and muscle contractions, directly or indirectly, controls DMP1 secretion along with FAM20C upregulation.”
“, body weight-associated mechanical loading triggers the mechanoreceptor PIEZO1 to enhance the production of FAM20C kinase in osteoblasts, which induces a burst in DMP1 secretion into ECM. Second, large amounts of extracellular DMP1 inhibit VEGF signalling in the OF and transform highly angiogenic type H vessels into quiescent type L vasculature to limit bone growth activity. In parallel, extracellular DMP1 leads to rapid matrix mineralisation and strengthening of long bones”
Reducing the levels of human DMP1 or it’s receptors may be a way to grow taller in adolesence and possible allow for new bone growth post skeletal maturity but more testing has to be done.
“The process of longitudinal bone growth occurs at the growth plate where the chondrocytes undergo apparent structural and molecular changes to promote growth. Recent reports suggest that radial shockwave treatment (rSWT) stimulates bone length in cultured fetal rat metatarsals. Therefore, we investigated if rSWT has similar growth promoting effects on cultured human growth plate fragments and addressed the same in a preclinical in vivo rabbit model by subjecting their growth plates to rSWT.
Short-term effects of high-energy rSWT were evaluated in a unique model of cultured human growth plate cartilage (n = 5) wherein samples exposed to rSWT were assessed for chondrogenic markers at 24 h in comparison to unexposed samples obtained from the same limb.
Local in vivo effects were studied in six-week-old rabbits{6 week old rabbits are about equal to 42 week humans which is very young} who had their distal femurs exposed to four weekly sessions of rSWT at low- and high-energy levels (n = 4 each){weekly sessions are not that much}. At sacrifice, histomorphometric and immunohistochemistry analyses were performed. For effect on longitudinal growth, proximal tibiae of 22-week-old rabbits (n = 12) were asymmetrically exposed to rSWT; the contralateral side served as untreated controls. At sacrifice, the final bone length was measured.
In the ex vivo model of cultured human growth plate cartilage, rSWT exposure upregulated SOX9 and COL2A1 compared to control.
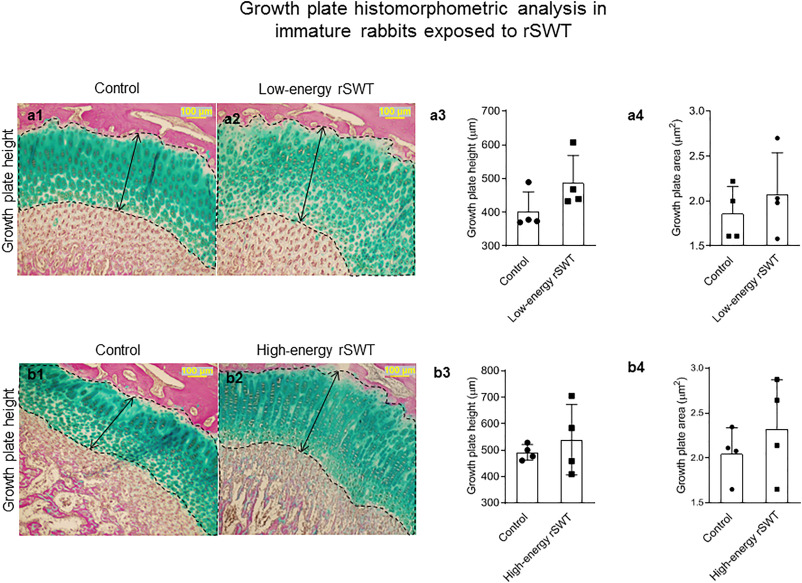
In the immature rabbit model, an increased number of proliferative chondrocytes and column density was seen for both the energy levels. In the adolescent rabbits, an increase in tibial length was observed after the fourth session of high-energy rSWT and until six-weeks after rSWT compared to the untreated limb.
Our preliminary experimental results suggest that rSWT may serve as a non-invasive treatment and possibly a safe strategy to stimulate longitudinal bone growth. However, further studies are needed to assess the in vivo effects of rSWT in models of disturbed bone growth.”
“22-week-old healthy rabbits (n = 12; 7 females, five males; weight 2.0–2.5 kg) was performed to document the effects of high-energy rSWT (3000 impulses, 180 mJ, 5 Hz) once weekly for four weeks on bone length. “
” Low-level laser beams and ultrasound are non-invasive modalities that have been investigated without success. Extracorporeal shockwave therapy (SWT) is a candidate for non-invasive modulation of growth plate activity as it has been successfully tested in fracture healing, nonunions, and other musculoskeletal disorders with minor complications in the clinic “
“After exposure to rSWT, gene expression analysis was performed after 24-h of culture. We observed increased expression of SOX9 (mean fold change: 3.0 ± 2.3) and COL2A1 (mean fold change: 19.0 ± 29.26) in treated samples when compared to untreated controls”
“he chondrocytes-column density (columns per mm growth plate width) in the proliferative zone was significantly increased in both the low-energy (low-energy rSWT: 40 ± 12 and control: 32 ± 9) and the high-energy rSWT groups (high-energy rSWT: 51 ± 13 and control: 37 ± 3)”
That looks like a pretty dramatic impact. Although shockwave also increased chondrocyte apoptosis so it’s possible that it increases growth rate but not total growth plate assisted height.
“At 26 weeks of age, after four sessions (at weekly intervals) of high-energy rSWT, there was a significant increase in the differences between the lateral tibial length measured on radiographs when compared to untreated controls (mean difference: 0.28 cm; p = 0.008). Six-weeks after the last session of high-energy rSWT the difference in the lateral tibial length treated bones compared to untreated controls was 0.03 cm (p = 0.001)” Rabbit tibial length may be about 10cm. So 0.28cm is like a 2.8% increase. Which is kind of significant.
” it is challenging to maintain this significant increase in bone length when dealing with healthy animals as the bone lengths tend to equalize after treatment withdrawal”<-so it may only affect growth rate not growth capacity.
So basically it’s worth studying but we don’t know if it only increases growth rate.
In some cases it’s worth noting extracorporeal shockwave therapy reduced length as seen above but of course the incidents were growth was increased is greater.
“Previous studies that used fSWT, a device used for its osteogenic effects, showed no effect on the growth plate cartilage in rats and rabbits”
“The high-energy rSWT used in the histological study did not cause cell death as measured with apoptotic markers and was considered safe for longitudinal bone growth experimentation.”
“one of the animals that received high-energy rSWT showed excess bone formation in the medial femoral condyle proximal to the growth plate in the metaphyseal region. This could be an adverse consequence of rSWT on periosteal cells proximal to the growth plate reflecting either increased vascularity or traumatic detachment of the periosteum. Therefore, careful evaluation needs to be considered when translating rSWT to patients as it may cause unpredictable excess growth akin to a metaphyseal fracture.”<-this is huge for us! We want excess bone formation!
Here is the excess bone formation in question:
That is pretty significant. 22 rabbits were used.
“When investigating the effects of high-energy rSWT, we found up to 1% increase in the final bone length in treated adolescent rabbits when considering the observations as paired data. An earlier study in rabbits using (piezoelectric device) focal extracorporeal shockwave therapy (fSWT) supports the growth stimulatory effect . Our study is different from the previous one in three ways. First, we used rSWT, which is safer because it generates less energy with low penetration than piezoelectric fESWT. Second, we exposed adolescent animals to rSWT and followed them until growth plate fusion to know if the changes in bone growth were sustained until the end of growth. Thirdly, we performed molecular and histological studies to demonstrate effects at the growth plate level.”
“observed stimulation of growth following rSWT could be due to cellular changes within the growth plate. It is plausible that the stimulated resting chondrocytes may have augmented the propagation of daughter cells during their subsequent entry into the proliferative zone, thus contributing to an increased columnar density”
Here’s a study that shows that extracorporeal stimulation can add bone to the hip:
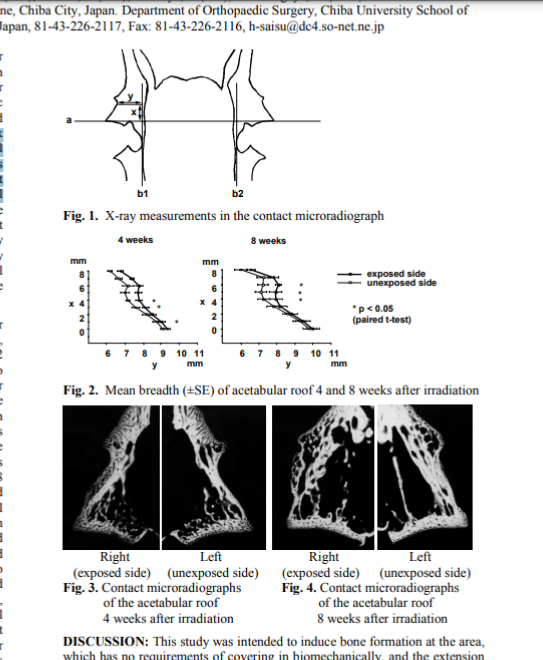
“We conducted this animal study to demonstrate whether exposing the acetabulum in immature rabbits to extracorporeal shock waves induces bone formation in the acetabulum. Five thousand shock waves of 100 MPa each were directed, from outside, at the acetabular roof of eight immature rabbits. At each of two time points (4 and 8 weeks) after treatment, the pelvises of four rabbits were removed and evaluated morphologically. Woven bone formation was observed on the lateral margin of the acetabular roof at 4 weeks after treatment, and the breadth of the acetabular roof in the coronal plane was significantly increased{coronal plane is basically length}. Eight weeks after treatment, the woven bone disappeared; the breadth of the acetabular roof, however, was significantly increased. These findings demonstrated that extracorporeal shock waves induced acetabular augmentation in rabbits. We conclude that extracorporeal shock waves, perhaps, could be applied clinically for the treatment of acetabular dysplasia.”
“No fracture was observed on the plain X- ray photo during the monitoring period after irradiation.”
“Extracorporeal shock wave therapy, which was developed for lithotripsy, is thought to be also useful to give dynamic loading to organs noninvasively. Shock wave demonstrates its physical action specific on bone as on calculus . It was reported that exposure to shock waves caused fracture of cancellous trabecula or periosteal lifting”
“Eight male New Zealand White rabbits aged 9 weeks weighing 1.0-1.2kg were used. Piezolith 2300 (Richard Wolf Inc., Germany) was used to produce extracorporeal shock waves. Ultrasonic waves were used for focusing. The focus was set in 3 mm cranial from superolateral edge of the acetabulum and 2 mm inside from lateral margin of the acetabular roof. Each 4 animals of the 8 animals were grouped into Group I and II. Shock waves were irradiated on the right acetabular roof from outside. The strength and the number of the shock wave were set to be 100 MPa and 5000 times respectively.”
“Certain exercises and stretches may help minimize leg length discrepancy and ease any related symptoms.”
“Physical force can cause micro strains on your bones, which results in incremental changes in bone mass and length — especially if the exercise is repeated over time. “
I’ve studied microstrain in the past and I believe that microstrain is a tool that can be used to make people taller. Either by alterations in the fluid forces in the bone, by inducing plastic deformation, complete trabecular microfractures resulting in endochondral ossification one trabeculae at a time, or piezoelectric forces modifying osteoclast and osteoblast activity.
“One exercise that can put this kind of strain on your affected leg bones is side kicking into the air. To get the most out of this exercise, do multiple sets daily.”<-Is side kicking into the air going to cause the right forces to induce height growth? I’m not one to discount any potential height increase method. But I would at least like to see some anecdotal evidence for this if not some kind of study. I don’t know if you could get animals to side kick in the air. And I think it would be hard for humans to get the right technique as you’d want the right kind of microstrain. I assume the goal would be tensile plastic deformation gradually lengthening the bone one microstrain at a time or piezoelectric forces altering osteoblast and osteoclast activity such that the bone is remodeled in a more lengthened state.
The article also mentions a quadriceps left and hamstring stretch which I do not think are related to lengthening bones.
Here are the sources mentioned in the study:
Arthritis and Rheumatology: “Brief Report: Leg Length Inequality and Hip Osteoarthritis in the Multicenter Osteoarthritis Study and the Osteoarthritis Initiative.”
European Cells and Materials: “Mechanical Loading and How It Affects Bone Cells: The Role of the Osteocyte Cytoskeleton in Maintaining Our Skeleton.”
International Research Journal of Engineering, IT & Scientific Research: “Relationship between length of leg and strength of leg muscle to frequency of straight kicks.”
Journal of Athletic Training: “Standing and Supine Hamstring Stretching Are Equally Effective.”
Journal of International Medical Research: “Post-THA gait training to improve pelvic obliquity and decrease leg length discrepancy in DDH patients: a retrospective study.”
From Mechanical Loading and How It Affects Bone Cells: The Role of the Osteocyte Cytoskeleton in Maintaining Our Skeleton, “”1,000 microstrain equals a 0.01 % change in length of the bone compared to its original length. Vigorous exercise induces bone strains up to 1,000 microstrain in humans.”<-but this will only be a permanent increase in length if the 0.01% change in length is plastic. If the change in length is elastic it will return to it’s original length like a rubber band.
Cardarine has been used by bodybuilders and is linked to height growth. Cardarine is a PPAR Delta agonist(activator).
PPARDelta has been linked to height. From A single nucleotide polymorphism on exon-4 of the gene encoding PPARdelta is associated with reduced height in adults and children.“compelling evidence was found for this locus and its association with height (P = 10(-8)) with an overall effect size of about 0.5 cm per allele{1cm total}.” It’s possible that the effects of PPARdelta are biphasic where there is an equilibrium amount to maximize height and too little or too much reduces height or that there is a minimum amount of PPARDelta activation that is needed for height and that any further has no effect. The authors speculate that PPARDelta may affect height via metabolic efficiency or via affects on osteoclast function. Metabolic efficiency would have no effect on height as an adult but there is potential if it affects osteoclast function as degradation of bone would be a needed step to grow taller as an adult as it would both make the bone more susceptible to plastic deformation and allow for tissues that are capable of interstitial growth to take the place of bone.
Obviously, 1 cm in height is not going to break the bank in terms of increasing height while skeletally immature but if a PPARdelta agonist can increase osteoclast activity that can be used as part of a height increase routine.
Here’s the studies that says PPAR affects osteoclasts
“Osteoclasts modulate bone resorption under physiological and pathological conditions. Previously, we showed that both estrogens and retinoids regulated osteoclastic bone resorption and postulated that such regulation was directly mediated through their cognate receptors expressed in mature osteoclasts. In this study, we searched for expression of other members of the nuclear hormone receptor superfamily in osteoclasts. Using the low stringency homologous hybridization method, we isolated the peroxisome proliferator-activated receptor delta/beta (PPARdelta/beta) cDNA from mature rabbit osteoclasts. Northern blot analysis showed that PPARdelta/beta mRNA was highly expressed in highly enriched rabbit osteoclasts. Carbaprostacyclin, a prostacyclin analogue known to be a ligand for PPARdelta/beta, significantly induced both bone-resorbing activities of isolated mature rabbit osteoclasts and mRNA expression of the cathepsin K, carbonic anhydrase type II, and tartrate-resistant acid phosphatase genes in these cells. Moreover, the carbaprostacyclin-induced bone resorption was completely blocked by an antisense phosphothiorate oligodeoxynucleotide of PPARdelta/beta but not by the sense phosphothiorate oligodeoxynucleotide of the same DNA sequence. Our results suggest that PPARdelta/beta may be involved in direct modulation of osteoclastic bone resorption.“
Here’s the other study:
PPAR agonists modulate human osteoclast formation and activity in vitro
“Peroxisome proliferator-activated receptors (PPARs) are members of the nuclear steroid hormone superfamily and exist in three isoforms: PPARalpha, beta and gamma, each with specific functions. In this study, we have investigated the expression of PPARs by human osteoclast precursors and osteoclasts generated in vitro. In addition, the effects of fibrates and isoform-specific PPAR agonists on osteoclast formation and resorption in vitro were determined. Human peripheral blood mononuclear cells (PBMCs) were stimulated with human recombinant RANKL and M-CSF to generate osteoclasts. RNA was extracted at days 0, 7, 14 and 21 and RT-PCR for all three PPAR isoforms demonstrated their expression throughout this culture period. To determine the effect on osteoclast formation, PPAR agonists (10(-8) M to 10(-5) M) were added from the beginning of the culture until day 14 and the number of multinucleated osteoclasts counted. The effect of PPAR agonists on osteoclast function was similarly determined by treating mature, multinucleated osteoclasts cultured on dentine wafers with PPAR agonists (10(-8) M to 10(-5) M) for 7 days and quantifying resorption. Bezafibrate and fenofibrate, which non-discriminately activate all PPAR isoforms, significantly inhibited the formation of multinucleated osteoclasts from PBMC in vitro. Bezafibrate treatment of mature osteoclast resulted in 50% inhibition (at 10(-8) M and 10(-7) M) of resorption, yet fenofibrate had no significant effect. Activation of individual PPARs with isoform-specific agonist (GW9578, L165041 and ciglitizone which preferentially activate PPARalpha, beta and gamma respectively) resulted in significant dose-dependent inhibition of multinucleated osteoclast formation. Divergent effects on osteoclast resorption were observed; GW9578 had no significant effect on resorption, whereas ciglitizone and L165041 dose-dependently inhibited and stimulated resorption, respectively. These data show for the first time expression of all three PPAR isoforms throughout the development and maturation period of osteoclasts generated from human PBMCs. In addition, we demonstrate that isoform-specific PPAR agonists have strong effects on multinucleation and highly variable effects on bone resorption. In conclusion, this study highlights the potential of PPARs as therapeutic targets in diseases with accelerated osteoclast formation and resorption.”
I couldn’t find any further studies linking PPARDelta to longitudinal bone growth nor can I find any anecdotal cases of people growing taller off of taking cardarine.
Arthur Lazar is someone who has spoken about LSJL in the past on Quora. “Not really. There is 0 evidence for that. The original working experiment was performed on mice – mice growth plates never ossify. MAYBE if someone would develop a machine which can put perfect constant pressure, perfectly shaped for bone area where the pressure is supposed to be, then in theory it could work. But this is a bro-science, so it’s a big MAYBE. But as for now, using clamp, dumbelss or whatever you can use to press at bone would never work.”<-Mice growth plates don’t ossify but they become senescent which is just as bad for growth.
Here’s some more of his thoughts on LSJL: “Yes, I do work on a device for automatic long bone loading method as I believe that the standard lsjl loading (manual with clamps, weights, mpistols) is an invalid approach that lacks consistency, frequency and stability which all was provided with the original, successful experiment.”<-I don’t know what an mpistol is. I believe it is a typo. I don’t know what the original intent is.
“Thank you for your interest, but currently my team is complete and current priority of the projects puts the lsjl idea on the bottom of the list. When I am done with the prototype and IF it will have a desired affect on Flexioss structure (in the terms of force application on the structure) I will publish the design in order to expand the team and get potential investors interested.”
So the question is should we be using flexioss to try to find the best loading regime to induce the proper stimulation to induce new longitudinal bone growth. I believe personally that the best regime is some kind of lateral impact loading(I believe that tapping the epiphysis would be superior than the diaphysis now but I am trying both). Clamping has a slippage problem which impact does not have. The loads of direct lateral impact are stronger than that occur during normal physiological activities which are more axial.
Lateral impact does occur during boxing both to the hand and to the face and ribcage. Also, it occurs to the feet bones during running(but this depends on whether you are a heel or toe striker). It also happens to bones during muay thai kick boxing.
The problem is that this impact is often at irregular intervals and not targeted to specific areas of the bone such as the epiphysis. The epiphysis is where there is less cortical bone, is close to where the growth plates used to reside in skeletally mature individuals, and is close to the articular cartilage which if stimulated could potentially contribute to height growth. In muay thai you have no control over where you are kicked and if you do kick you are trying to use the strongest part of the bone.
Lateral impact has the potential in my opinion to drive the most fluid forces throughout the bone. Greater than any axial impact certainly due to the pressure gradient of the bone and the epiphysis is the weakest most porous part of the bone so impact to that area has the potential to drive fluid forces throughout the entire bone. Muscular contractions also have the ability to stimulate fluid forces throughout the bone but that is limited by muscular size and strength. Lateral impact also has the ability to gradually induce plastic deformation throughout the bone. Most plastic deformation occurs axially to shorten the bones such as in rickets/paget’s disease etc. Lateral impact loads have the potential to induce plastic deformation in a way such as to lengthen the bones.
So the question is can we use the flexioss to find the best way to induce lateral plastic deformation in such a way as to lengthen the bones or to induce fluid forces to either induce articular cartilage endochondral ossification or to cause denovo cartilagenous regions within the bone.
The manufacturers of flexioss claim that it has properties similar to that of cancellous bone so yes it can potentially be used to find the best loading regime to induce plastic deformation in such a way as to longitudinally lengthen the bone. Obviously, it can’t really be used to mimic the fluid properties of the bone.
I have tried the McKenzie Chin Tuck posture and it absolutely makes you measure taller but your eye level appears shorter. It is not a breakthrough by any means but I have tried and you can see yourself becoming taller in the mirror when you do it.
So when you adopt this posture you measure taller because you are maximizing the apex bump of your head. But personally, I feel shorter because with a more backwards head posture my eyes are at a higher level so people are shorter relative to high level.
There is an exercise related to this where you push the chin back to get a neck muscle stretch and there are some indications that it may be worthwhile to do this.
I write more in my response to Body Height changes with hyperextension. Basically temporary hyperextension of the spine(15s) can result in temporary height gain due to disc hydration. And I think this exercise may achieve hyperextension of disc components. So I’d say it’s worth doing but only brief periods as you would be better suited to strengthening your neck muscles via something like free weight training or machines if you can’t do free weights due to injury or a structural reason.
It’s mentioned further in the body height changes with hyperextension study that it’s putting the load on the facets that enables for disc hydration. You’d think that tilting your head back would actually put the load on the facets. But I think the key is that tucking your chin in achieves neck muscle activation and if you look at the back muscle anatomy if the muscles are activated they will pull everything upwards.
Note that the majority of the back muscles slope upwards so when they are contracted they indirectly pull up the spine in alignment. I write about the muscular pull maximizing height gain here.
So I’d say in general adopt the mckenzie chin tuck along with chest up/shoulders back to maximize back muscle activation in posture. And occasionally do the press the finger against the chin thing for short periods of time to allow for disc hydration.
The drawback for the mckenzie chin tuck posture is that although it makes you measure taller it makes your jaw look smaller.
Here’s a video that explains it more:
I find that just bringing your chin is enough to get a good height gain appearance without having to worry about protecting the technique yes as mentioned you will have double chins but you will measure taller.
This guy looks taller after doing the McKenzie chin tuck:
Here’s a study that backs up the McKenzie chin tuck:
Head posture and loading of the cervical spine
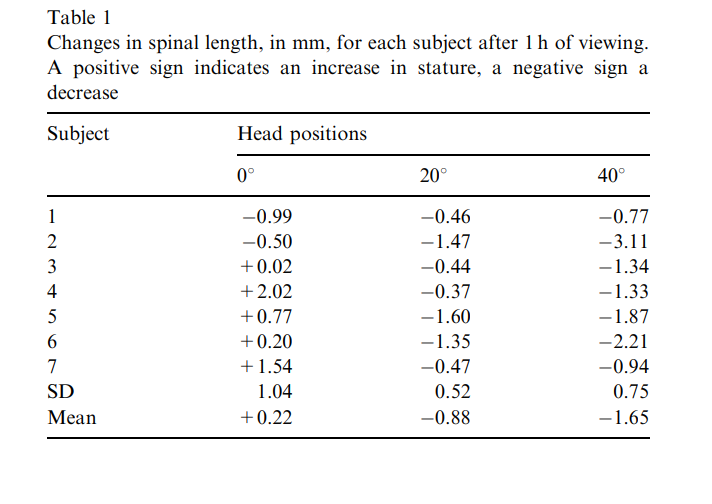
” Precision stadiometer tests were run, using seven subjects, to measure the effects on spinal length of different angles of gaze. After 1 h exposure whilst sitting in a controlled posture, there were significant differences in the shrinkage of the spine between the horizontal gaze and the 20° and 40° angles below the horizontal. The increased spinal loading demonstrated by the increase in spinal shrinkage calls into question the recommendations for angle of gaze recommended in textbooks.”
I think it is the forward posture affecting the height change and not actually the gaze of the eyes.
“The mean compressive load on the cervical discs was 10 kg higher for the forward flexed position”
“Each subject would attend on three separate days, on each of which one of the three randomly chosen head angles, 0 degree, 20 degrees and 40 degrees, would be tested.”
“A shrinkage of the spine during the forward inclination of the head, observed during this experiment, of approximately 1 mm over a 1 h period, equivalent to about 5% of the total diurnal shrinkage”