I remember reading from a baby rearing book once that the mother’s breast milk contains all of the natural needed nutrients for a human baby to grow. We know from research that babies who are not well treated or taken care of early in their life during their baby and toddler years are less likely to develop properly stunting their growth. That is the psychological element to the baby rearing for optimum growth. However, I wondered whether it is also helpful from a dietary point of view for optimum height growth to extend the breast feeding stage. I am not suggesting that the developing toddler only have human breast milk but use that as a supplement to their already diet of nutritious food for increased growth during those critical baby years.
I would even suggest that after the child has grown too old for breast feeding, they should still be getting synthetic human milk for ingestion because the nutrients inside it is so potent and wholesome. I doubt there has been any studies done but I would be willing to guess that children who has had extended amount of time with breast feeding may grow up to be more fitter , thus taller, than their peers who did not get the extra human breast milk.
If it was more accept in more modern developed nations, I would suggest replacing the milk of bovine (cow) with human milk for height increase purposes since it seems to be more appropriate for humans and have a better match for the human body’s needs.
UPDATE: I guess I was proven wrong and that there has been already a few studies done that showed that breastfeeding shows an increase in growth of bone length. The studies can be found HERE, and HERE.
The benefits of the mother’s breast milk is too great to describe so I wanted to list the benefits and composition of it from Wikipedia (source HERE).
Breast milk, to be specific human milk, is the milk produced by the breasts (or mammary glands) of a human female for her infant offspring. Milk is the primary source of nutrition for newborns before they are able to eat and digest other foods; older infants and toddlers may continue to be breastfed, either exclusively or in combination with other foods.
According to a report by msnbc.com released online on Saturday, June 30, 2012, human breast milk may have the ability to act against, and to possibly kill, HIV (the human immunodeficiency virus), the virus that ultimately causes AIDS (Acquired Immune Deficiency Syndrome). The study was carried out at the University of North Carolina Center for Infectious Diseasesand the University of North Carolina Center for AIDS Research, but will need to be replicated in other clinical and laboratory studies at other institutions, such as other hospitals and universities, to be considered as admissible scientific evidence, not least because a claim that a bodily fluid can kill the AIDS virus would be considered a scientific novelty and breakthrough of large proportions (human breast milk can also transmit the virus).[2]
The baby nursing from its own mother is the most ordinary way of obtaining breastmilk, but the milk can be pumped and then fed by baby bottle, cup and/or spoon, supplementation drip system, and nasogastric tube. Breastmilk can be supplied by a woman other than the baby’s mother; either via donated pumped milk (for example from a milk bank), or when a woman nurses a child other than her own at her breast — an ancient and storied practice known as wetnursing.
The World Health Organization recommends exclusive breastfeeding for the first six months of life, with solids gradually being introduced around this age when signs of readiness are shown. Supplemented breastfeeding is recommended until at least age two and then for as long as the mother and child wish.[3]
Breastfeeding continues to offer health benefits into and after toddlerhood.[4] These benefits include a somewhat lowered risk of Sudden Infant Death Syndrome (SIDS),[5] increased intelligence, [6]decreased likelihood of contracting middle ear infections,[citation needed] cold and flu bugs,[citation needed] a tiny decrease in the risk of childhood leukemia,[citation needed] lower risk of childhood onset diabetes,[citation needed] decreased risk of asthma and eczema,[citation needed] decreased dental problems[citation needed] and decreased risk of obesity later in life,[7] and may possibly include a decreased risk of developing psychological disorders, particularly in adopted children.[8][9]
Breastfeeding also provides health benefits for the mother. It assists the uterus in returning to its pre-pregnancy size and reduces post-partum bleeding, as well as assisting the mother in returning to her pre-pregnancy weight. Breastfeeding also reduces the risk of breast cancer later in life.[10]
Under the influence of the hormones prolactin and oxytocin, women produce milk after childbirth to feed the baby. The initial milk produced is often referred to as colostrum, which is high in theimmunoglobulin IgA, which coats the gastrointestinal tract. This helps to protect the newborn until its own immune system is functioning properly, and creates a mild laxative effect, expellingmeconium and helping to prevent the build-up of bilirubin (a contributory factor in jaundice).[edit]Production
Actual inability to produce enough milk is rare, with studies showing that mothers from developing countries experiencing nutritional hardship still produce amounts of milk of similar quality to that of mothers in developed countries.[11] There are many reasons a mother may not produce enough breast milk. Some of the most common are an improper latch (i.e., the baby does not connect efficiently with the nipple), not nursing or pumping enough to meet supply, certain medications (including estrogen-containing hormonal contraceptives), illness, and dehydration. A rarer reason is Sheehan’s syndrome, also known as postpartum hypopituitarism, which is associated with prolactin deficiency; this syndrome may require hormone replacement.
The amount of milk produced depends on how often the mother is nursing and/or pumping; the more the mother nurses her baby, or pumps, the more milk is produced.[12][13][14][15][16] It is very helpful to nurse on demand – to nurse when the baby wants to nurse rather than on a schedule. If pumping, it is helpful to have an electric high-grade pump so that all of the milk ducts are stimulated. Some mothers try to increase their milk supply in other ways – by taking the herb fenugreek, used for hundreds of years to increase supply[17] (“Mother’s Milk” teas contain fenugreek as well as other supply-increasing herbs); there are also prescription medications that can be used, such as Domperidone (off-label use) and Reglan.[18]
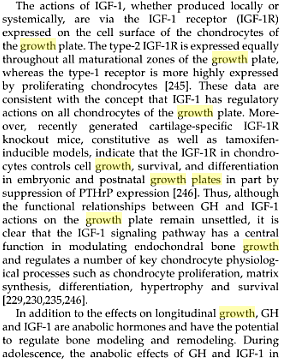
Composition
Composition of human breast milk
| Fat |
| total (g/100 ml) |
4.2 |
| fatty acids – length 8C (% ) |
trace |
| polyunsaturated fatty acids (%) |
14 |
| Protein (g/100 ml) |
| total |
1.1 |
| casein 0.4 |
0.3 |
| a-lactalbumin |
0.3 |
| lactoferrin (apo-lactoferrin) |
0.2 |
| IgA |
0.1 |
| IgG |
0.001 |
| lysozyme |
0.05 |
| serum albumin |
0.05 |
| ß-lactoglobulin |
– |
| Carbohydrate (g/100 ml) |
| lactose |
7 |
| oligosaccharides |
0.5 |
| Minerals (g/100 ml) |
| calcium |
0.03 |
| phosphorus |
0.014 |
| sodium |
0.015 |
| potassium |
0.055 |
| chlorine |
0.043 |
The exact integrated properties of breast milk are not entirely understood, but the
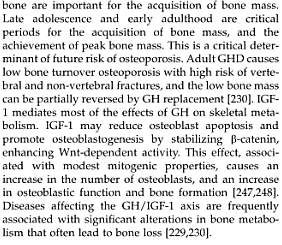
Storage of expressed breast milk
Expressed breast milk can be stored for later use. It is recommended that the milk be stored in hard-sided containers with airtight seals. Some plastic bags specifically manufactured for the storage of expressed breast milk are designed for storage periods of less than 72 hours – others can be used for up to 6 months if frozen.[32] The amount of time that it can be safely stored for use by infants in a home-based situation is given in this table.[33]
| Place of storage |
Temperature |
Maximum storage time |
| In a room |
25°C |
77°F |
Six to eight hours |
| Insulated thermal bag with ice packs |
|
|
Up to 24 hours |
| In a refrigerator |
4°C |
39°F |
Up to five days |
| Freezer compartment inside a refrigerator |
-15°C |
5°F |
Two weeks |
| A combined refrigerator and freezer with separate doors |
-18°C |
0°F |
Three to six months |
| Chest or upright manual defrost deep freezer |
-20°C |
-4°F |
Six to twelve months |
Comparison to other milks
All mammalian species produce milk, but the composition of milk for each species varies widely and other kinds of milk are often very different from human breast milk. As a rule, the milk of mammals that nurse frequently (including human babies) is less rich, or more watery, than the milk of mammals whose young nurse less often. Human milk is noticeably thinner and sweeter than cow’s milk.
Whole cow’s milk does not contain sufficient vitamin E or essential fatty acids. Whole cow’s milk also contains excessive amounts of protein, sodium, and potassium, which may put a strain on an infant’s immature kidneys. In addition, the proteins and fats in whole cow’s milk are more difficult for an infant to digest and absorb than the ones in breast milk.[34] Evaporated milk may be easier to digest due to the processing of the protein but is still nutritionally inadequate. A significant minority of infants are allergic to one or more of the constituents of cow’s milk, most often the cow’s milk proteins.[35] These problems can also affect infant formulas derived from cow’s milk.
Alternative uses for breast milk
In addition to providing essential nourishment to infants, human milk; i.e., breast milk, has a number of valuable uses, especially medicinal uses, for both children and adults. It has been used medicinally for thousands of years.[36] The antibacterial and healing properties[citation needed] of breast milk are often overlooked, even by the nursing mothers themselves.[37] Breast milk contains strong antibodies and antitoxins that many people believe promote healing and better overall health. However, breast milk lacks sterile and antiseptic properties if a nursing mother is infected with certain communicable diseases, such as HIV and various bacterial infections like Group B streptococcus, as breast milk can transmit such diseases to infants and other people.[38]
Breast milk has been used as a home remedy for minor ailments, such as conjunctivitis, insect bites and stings, contact dermatitis, and infected wounds, burns, and abrasions. Breast milk has also been used alternatively to boost the immune system of ill persons having viral gastroenteritis, influenza, the common cold, pneumonia, etc., because of its immunologic properties. However, breast milk should never be seen or construed as a “cure-all”. Some medical experts are convinced that breast milk can induce apoptosis in some types of cancer cells. However, more research and evidence are needed in this area of cancer treatment.[39]
A minority of people, including restaurateur Hans Lochen of Switzerland and restaurateur Daniel Angerer of Austria, who operates a restaurant in New York City, have used human breast milk, or at least advocated its use, as a substitute for cow’s milk in dairy products and food recipes.[40] Tammy Frissell-Deppe, a family counselor specialized in attachment parenting, published a book, titled A Breastfeeding Mother’s Secret Recipes, providing a lengthy compilation of detailed food and beverage recipes containing human breast milk.[41] The animal rights organization known as PETA ignited a firestorm of criticism when it urged a dairy company to replace the cow’s milk they use in their ice cream products with human breast milk as a way to stop cattle abuse.[42][43] Human breast milk is not produced or distributed industrially or commercially, because the use of human breast milk as an adult food is considered unusual to the majority of civilized cultures around the world, and most disapprove of such a practice.[44]
Attempts to formulate soap from breast milk have also been made, and those using it claim that its effectiveness as a cleanser is greater than, or equal to, that of traditional soaps.[45]
Passing of unwanted substances
Despite the risk of substances transmitting from the mother to the child through breast milk, breastfeeding has far more advantages than infant formulas, and, with few exceptions, the WHO recommends exclusive breastfeeding for the first 6 months of life.[46]
The milk-producing cells are most permeable to drugs during the first postpartum week.[47]
Drug characteristics that increase excretion in milk include:[47]
- Not plasma protein binding
- Non-ionized
- Low molecular weight
- Lipid solubility rather than water solubility
- Weakly alkaline rather than weak acid
Drugs are transferred from blood plasma across ductal cells to the milk by diffusion or active transport. The latter may result in higher concentration of the drug in the breast milk than in the plasma of the mother.[47]
The amounts of most drugs in milk do not exceed 2% of the total ingested dose.[47]
Environmental pollutants
Environmental pollutants found in breast milk are usually not harmful, and should be considered only when environmental levels are unusually high. In addition, there has been a decrease in environmental levels, also resulting in a decrease breast-milk levels. Pollutants that are of most concern are pesticides, organic mercury, and lead. DDT and dieldrin are unavoidable, and can also be detected in infant formulas.[48] Pesticides and other toxic substances bioaccumulate; i.e., creatures higher up the food chain will store more of them in their body fat. This is an issue in particular for the Inuit, whose traditional diet is predominantly meat. Studies are looking at the effects of polychlorinated biphenyls and persistent organic pollutants in the body; the breast milk of Inuit mothers is extraordinarily high in toxic compounds.[49]
Extraordinary consumption
Spanish king Alfonso XIII visited the region of Las Hurdes in 1922 in order to display the concern of the crown. The king and his retinue lived in military tents planted near the town of Casares de las Hurdes. During the king’s visit, a strange incident took place: A local village chief, concerned that the king was drinking only black coffee (a consequence of the king’s aides distrusting the quality of the local milk owing to unsanitary conditions in the area), served the king a small jug of milk saying, “Your Majesty rest assured that this milk is totally trustworthy,”[50] which turned out to be breast milk from his wife who had recently given birth. The king became aware of this fact only after having had his café con leche.[51]
Preliminary research indicates that breast milk can induce apoptosis in some types of cancer cells.[39] Adults with GI disorders and organ donation recipients can also benefit from the immunologic powers of human breast milk.
In Costa Rica, there have been trials to produce cheese and custard from human milk as an alternative to weaning[52]
A controversial Swiss restaurateur has created a menu based around foods cooked in human breast milk.[53]
An Icecreamists in London’s Covent Garden started selling an ice cream named Baby Gaga in February 2011. Each serving costs £14. All the milk was donated by Mrs Hiley who earns £15 for every 10 ounces and calls it a “great recession beater”.[54] The ice cream sold out on its first day. Despite the success of the new flavour, the Westminster Council officers removed the product from the menu to make sure that it was, as they said, “fit for human consumption.”[55]