FINITE ELEMENT ANALYSIS OF AN UNDER-ACTUATED ROBOTIC DEVICE FOR
KNEE LOADING APPLICATIONS
“Knee loading is one form of joint loading modalities, which potentially provides a therapeutic regimen to stimulate bone formation and prevent degradation of joint tissues. Healing of knee injuries is sensitive to many environmental stimuli. Since mechanical stimuli are crucial for the growth, development, and maintenance of articular cartilage and bone, we have developed an innovative robotic knee loading device to achieve this goal. This device induces mechanical loading to stimulate articular cartilage and bone, and it potentially reduces the healing time of injuries such as bone fractures. The robotic device is an improved version over previous joint loading devices, in which loads are applied at specific points with non-uniform loading around the knee joint. In this paper, finite element analysis (FEA) of this robotic device has been presented that includes static structural analysis and modal frequencies of the device for two different material configurations used in the design. The design with ABS plastic material offers the desired margin of safety while reducing the weight and cost. ”
“The robotic device examined in this paper is designed for small levels of deformation. The intended displacement of the working device is small, a maximum of 13 mm. large
deformations are not recommendable as such deformations will critically affect the effective range of motion of device. “<-we may want larger deformations for our purposes.
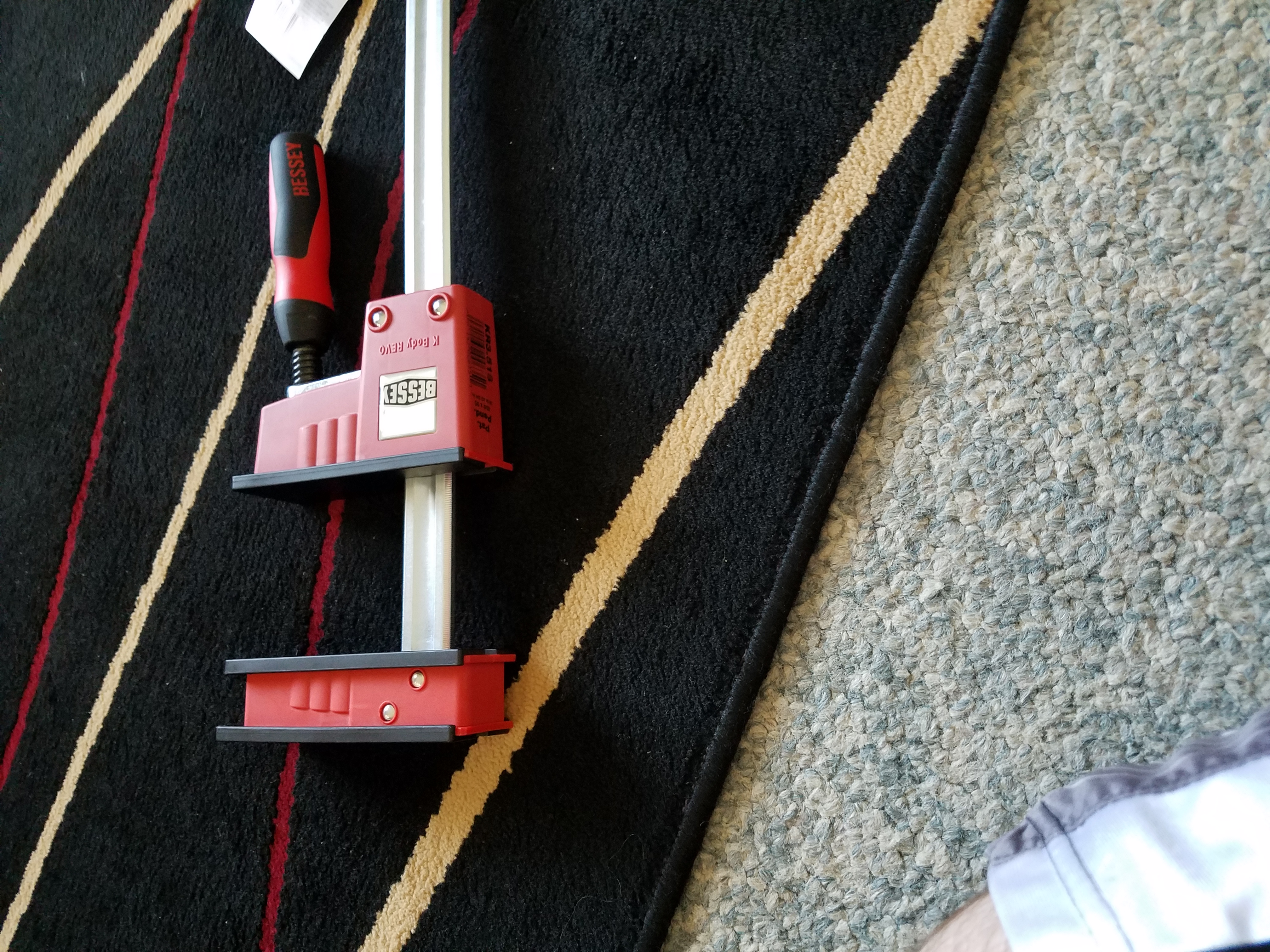
” If the stresses are too high for the material selected, the device may yield, resulting in the failure of the device.”<-this can happen with a clamp without enough strength.”
” if very small magnitude of mechanical stimuli is applied fast enough then it may induce a cellular response”<-This is an interesting thought. It’s very hard to produce a rapid mechanical stimuli physiologically. How many bicep curls can you perform in one second?
“Osteocytes are the highly mechanosensitive cells which senses the resulting physical stimuli from mechanical forces applied on bones. They constitute of more than 90% of bone cells.
When rapid mechanical loading is applied at the end of long bone, the interstitial fluid present around the osteocytes pressurizes causing the fluid flow which creates hydrostatic
pressure throughout the bone. This hydrostatic pressure excites the osteocytes resulting in enhanced osteogenesis which decreases the healing time of the fractures, increases the bone density and will be helpful in treatment of osteoporosis and osteoarthritis”<-we want additional stimuli from the hydrostatic pressure we want hydrostatic pressure to degrade bone tissue reducing the constraining effect that bone tissue has on growth and we want the stem cells to become more fibrocartilagenous.
“To apply such a load, a device would need to have a means of producing a transverse force directly to the end of a long bone, such as at the knee. A cyclic force applied in such an area would force a slight shift of the fluid within the bone towards the opposite end of the bone in a controlled fashion”<-this is what we do with the clamp. Produce a transverse(lateral) force directly to the end of a long bone. It has the potential to be cyclic if you rotate and reverse the rotation of the clamp. We may want more than a slight shift of fluid and we may not care if it’s in a controlled fashion or not.
“a maximum force of 40 N with the frequency range of 1 Hz to 5 Hz will have a promising effect on a human knee”<-Higher force may be needed for longitudinal bone growth.
” the efficacy of stimulating the osteocytes depended on the stress distribution on the knee. Based on this observation, it is projected that a position specific loading that provides a more
targeted force application on the knee is likely to further improve the efficacy of bone stimulation. It is hypothesized in that this targeted loading would contribute to the
improvement of new bone formation over a distributed loading modality. “<-maybe a smaller clamp pad and instead of clamping the knee as a whole clamping different epiphysis’ separately. Although we don’t necessarily care about stimulating the osteocytes, we want to degrade bone tissue and stimulate stem cells. The statement about more targeted loading still applies.
I can’t post an image of the device but look at fig 4 and 5.
” It can be seen that when maximum force of 20 N is applied on human knee, the maximum stress generated is 11.22 MPa. “<-Since around 10MPa is the chondrogenic stimulatory range this is a key pressure however you may need to degrade bone tissue as well. The study does not indicate exactly where in the knee the stress was generated. This was for alluminum and steel. Other materials were used and they were all in this same range.
FINITE ELEMENT ANALYSIS OF AN ELECTRO-MECHANICAL KNEE LOADING DEVICE
“When a cyclic but controlled load with a specific frequency is applied to the bones (femur and tibia) and surrounding tissues in the knee, it affects the osseous tissue causing physical deformations. These deformations result in pressure gradient in the intramedullary cavity of the bone. Due to this pressure difference, there is a fluid flow of molecules and nutrients.
This will result in osteoblast differentiation; a phenomenon will initiate new bone formation or osteogenesis. This can be used as a healing technique in case of bone related injuries
like fractures or diseases like osteoarthritis and osteoporosis.”<-slightly more powerful prediction in this study where they predict osteoblast differentiation and physical deformations. They mention a specific frequency being needed.
“When the device is loaded with a human knee, the inertial load resisting the driving force is considerable.”