This is a FAQ about the vibration and hammer method that I talked about in this youtube video.
Q: I’m worried about doing vibration because of jackhammer workers and hand-arm vibration syndrome?
A: The key word here is jackhammer. And the people who do jackhammers do them for hours a day. Vibration is a biphasic stimulus with too low duration giving new results and too high stimulus potentially causing nerve damage. The key is to find that happy medium. I do not think the highest setting is needed. Obviously, all vibration is not bad as you are exposed to vibration in moving vehicles for example. Ideally, we would have studies to determine the optimal vibration setting but I do not have the capability to do such studies.
Q: What things should you watch out for when performing vibration?
A: Tingling sensation in fingers, skin damage. If you get tingling sensation than adjust your method and shorten the duration. If you get skin damage then try holding the hammer in a different location to give your skin a break. Try to use “common sense”. Also, you can try some gloves or other skin protection while holding the hammer.
Q: What is the science behind the vibration + hammer holding method?
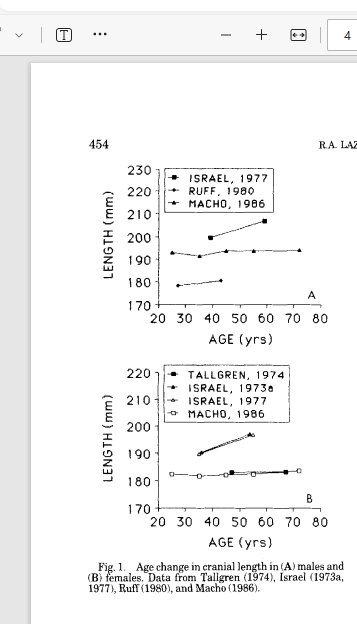
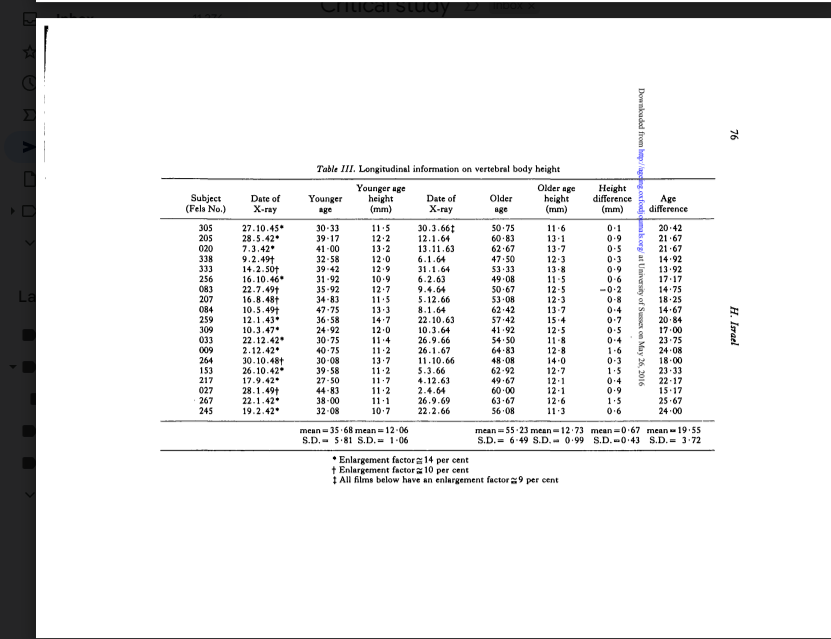
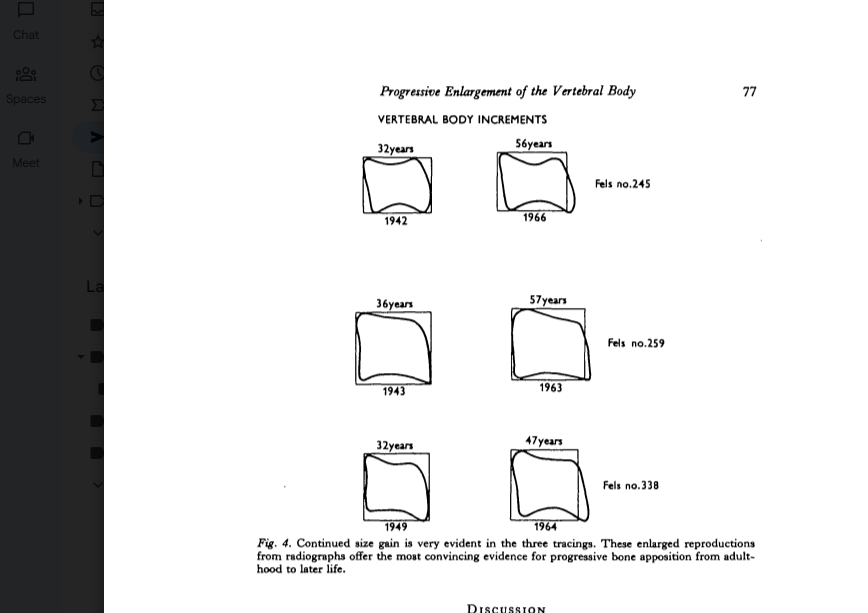
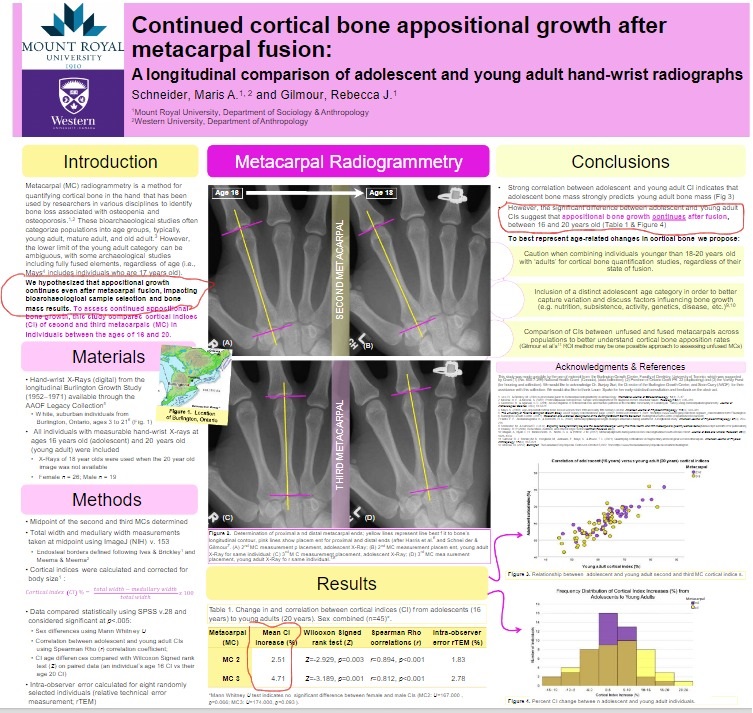
A: It is based on the anecdotal evidence that exercises such as archery, arm wrestling, and tennis have both been reported to increase bone length and they involve torsion and vibrational loading. Judo and baseball pitch mainly involve torsional loading and also have anecdotal evidence to increase bone length. Susan Pfeiffer’s paper Age Changes in the External Dimensions of Adult Bone have evidence that increase in bone length is possible post epiphyseal fusion. Torsional loading is the most effective way to drive fluid flow in the bone as what’s the best way to wring out a sponge? By twisting it. And vibrational loading further drives fluid flow. This fluid flow stimulates osteocyte activity. The exact mechanism by how this could increase bone length is yet unknown. But osteocytes have the power to drive both osteoblast and osteoclast activity so there could be a bone modeling effect where bone models to grow longer. It’s also possible that there could be a stem cell mechanism, plastic deformation, or articular cartilage endochondral ossification.
Q: How much have you grown from this method?
A: From self measurement I have increased my wingspan from 75 to 75 3/16″. I am only doing the method on my left hand and my left thumb seems much longer than my right thumb. Once I consistently measure 75 1/4″ the plan is to get x-rays. Wingspan is more accurate as you can do certain rotational tricks to make one hand appear longer than the other. Wingspan is reliable but there is variance so I measure multiple times. But any PR in wingspan is likely not measurement error as 1/16″ of an inch may as well be a mile as it is basically impossible to stretch your way to additional length. I need sufficient length as photoshop/gimp measurement is not 100% accurate so need to get above measurement error. I do have before X-rays.
Q: Has anyone else grown from this method?
A: Someone else has tried it and they have reported a growth in wingspan of 1/4″. They are doing it on both hands. I need other people to validate results because of measurement bias from myself.
Q: What’s the exact mechanism of performing the method?
A: I want people to use a variety of different techniques and use common sense. I do not think the exact vibration location and the exact mechanism of holding the hammer matters as the vibration and load is going to go throughout the entire hand. I do think though it’s better to do shorter durations, heavier loads(Hold hammer at end so it’s harder and there’s more torsion), possible hold multiple or heaver hammers, and do it multiple times during the day. Experimentation would be needed but I’m guessing the optimal duration would probably be 30 seconds to a minute multiple times during the day.
Q: I want to lengthen my legs and torso.
A: I have tried applying vibration and holding weights with feet and between knees. The issue is that legs are not as good as gripping things as the hands. Once this method is proven to work then we will have more resources and I can more easily test the other methods and have more support. So it is very important that even if you only want to grow legs you should try this method so I can get proof and then it will be easier to develop additional methods.
Q: I just want to do limb lengthening surgery.
A: The bones are connected to the tendons via the enthesis and any method that stimulates bones will likely stimulate the growth of those soft tissue as well due to the connection. People with limb lengthening surgery do seem to have issues with muscle tightness and bone healing post surgery. Vibration and torsional stimuli likely can help with this healing. So even if you only want to do surgery these techniques can possibly help with rehab. Also, it would be cost prohibitive to increase hand/foot size with limb lengthening surgery. This technique could be a cost efficient way to stimulate those tissues.
Q: Any supplements that can help?
A: I would recommend bone both soup for the hyaluronic acid and glucosamine/chondroitin. Also, a multivitamin. In the future, I can see things that stimulate CNP, HGH, IGF2, and Relaxin possibly helping as well.
Q: How fast can I expect results?
A: Results will vary but I’d say about 1/16″ per month.
Q: What will grow?
A: Fingers, palm, and possible overall arm length and width. It’d be hard to say for sure without more experimentation.
Q: I’m not getting results.
A: Try using a heavier hammer. Doing it more times during the day and increasing duration.
Q: Anyway to contact for further help?
A: Mail me at NaturalHeightGrowth@gmail.com or DM me at heightquest on instagram.