I was doing research on a completely unrelated subject just today and I came across a device that I have been doing research for (something else) and something that was written in the Product Description made me take a small step back and I realized something that I should have seen months ago. It was like a lightbulb went off in my head and I managed to connect 5 separate ideas into 1, sort of like how Edward Witten managed to take the 5 main string theory ideas developed by teams of theoretical physicists over multiple decades and both realize that all 5 developed ideas were all looking in a different way at the same, more unified superstring theory, as well as be able to integrate them all together into the M-Theory (it’s a physics reference). It is similar to the Jain idea of Anekantavada which suggest that often when different, multiple theories and view points are in conflict in being able to accurately describe something, the conflict may be from viewing the same phenomena in different points of views.
Most people are familiar with the idea of massagers, but I would guess that less people are familiar with a subset of massagers known as electronic pulse massagers. These massagers functions not through vibrating at high speeds to apply mechanical force to a body part, but by transmiting electrical current through the human body, specifically the muscle groups to get the muscles to contract and/or extend themselves. The goals of most massagers is to decrease pain, eleviate muscle tension, improve circulation, and help with certain chronic conditions.
The exact device I was looking at and studying was a type of Pulse Massager, one that operated on both the EMS and TENS theory. EMS theory works on stimulating muscle tissue, while TENS theory work on stimulating nerve endings.
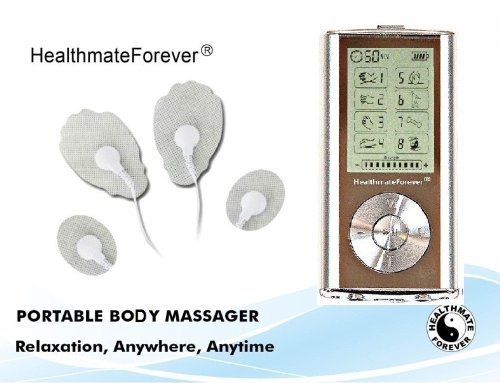 The actual product is called a Portable Body Massager sold by a company called HealthmateForever. It operates on two principles that is like a combination between Eastern Medicine and Western Medicine.
The actual product is called a Portable Body Massager sold by a company called HealthmateForever. It operates on two principles that is like a combination between Eastern Medicine and Western Medicine.
The Amazon webpage for this product states…
“…applying the modern electronic TENS and EMS simulation technology to improve the micro circulation of the human body, promote the absorption of inflammatory substances, relieve the tissue adhesion, and alleviate pain…”
So these strange subset of massagers known as pulse massagers operate by sending electrical signals to areas of the body. While most pulse massagers only operate on the EMS theory, which is just to stimulate the muscles, this model and design seems to operate also on the TENS model, which stimulates neural tissue, specifically the nerve endings. The one section that got me more curious was the claim made that this device can remove inflammatory substances and improve microcirculation.
Part #1: The theory of EMS and TENS
EMS (Electrical Muscle Stimulation) – From the Wikipedia article on this idea, it is also called neuromuscular electrical stimulation (NMES) or electromyostimulation. The idea is to have a main controller device that sends electrical pulses to an electrode pad attached to a body causing the muscles in the area to contract. The electrical signals is to replicate the electrical potential that goes through the body to signal muscle contraction.
TENS (Transcutaneous Electrical Nerve Stimulation) – This theory refers to the idea of sending electrical signals to the nerves of a person to for healing purposes. The devices currently sold in the market today are rather smaller and apparently you can control and change the pulse width, frequency and intensity of the electrical signal sent. From the Wikipedia article it states “Generally TENS is applied at high frequency (>50 Hz) with an intensity below motor contraction (sensory intensity) or low frequency (<10 Hz) with an intensity that produces motor contraction”
It is important to note that the devices that use either or both the EMS or TENS method look very similar and many people get these two theories mixed up. the thing to remember is “TENS is for blocking pain through stimulating nerve endsing, while EMS is for stimulating muscles to contract.”
Now, this is the first part of the puzzle. Keep reading to get all the pieces.
Part #2: The Interesting, almost EXPLOSIVE breakthrough research done by Dr Robert O. Becker
Dr. Robert O. Becker was a very controversial figure. He was a real doctor, who was an orthopedic surgeon with SUNY, Syracuse (from Wikipedia) as well as Director of Orthopedic Surgery at the Veterans Administration Hospital of New York, Syracuse. His controversial research was in a field known as electrophysiology aka electromedicine aka bioelectricity. Here are the list of things he did research on.
- Bone growth and bone fracture non-union healing acceleration – His bone studies are the ones that we are most interested in. He noticed that with bones that were in non-union, 1 nano ampere DC current greatly improves bone fusion.
- Accelerated Bone Healing: (Study: Dr. Robert Becker, et al., “Experience With Low-Current Silver Electrode Treatment of Nonunion,” in Electrical Prop. Bone & Cartilage (ed. C. T. Brighton, et al.), Grune & Stratton (1979), USA.) <— Note how Dr. Becker wrote this study with Dr. Brighton!
- Bone Growth: (Study #2: Dr. Robert Becker , et al., “Clinical Exp. With Low Intensity Direct Current Stimulation of Bone Growth,” Clin. Orthop. & Rel. Res., vol. 124, pp. 75-83 (1977) . USA)
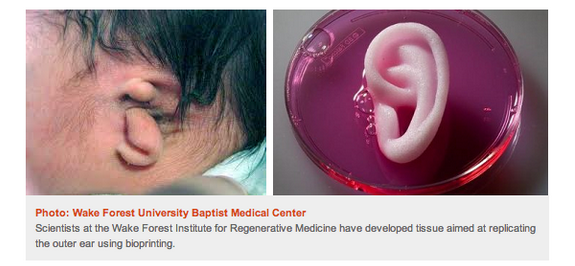
- Limb Regeneration – lower animals like salamanders had much better regeneration capabilities than frogs
- Connection between high power lines and cancer ocurrences – He was the guy who made the connection that high voltage lines can cause higher rates of certain types of cancers
- Unusual research into some fringe science ideas – the body’s electrical systems, hypnosis, visualization and acupuncture, parapsychology
- Regeneration technique in U.S. patent 70005556 – A silver electrode is placed upon a wound with the goal for a faster healing
- 2nd Patent – Iontopheretic system for stimulation of tissue healing and regeneration – US 5814094 A 1998 – He showed a way to stimulation tissue regeneration.
- Showed that each organism has a certain electrical potential – Which is now completely accepted in the scientific community. His work showed that living organisms and animals show a direct current of electric charge which is measurable from their body surface.
- (From the Wikipedia article on Dr. Becker) In the 1960s Becker’s research also showed that living bone can piezoelectrically generate electric potentials – led to work on using electricity in the treatment of ununited fractures. (Note: Ultimately, however, the use of electrotherapy for increasing bone healing has not been shown to be effective) <— This is one of the basic points behind why Tyler’s LSJL theory works, because the bones being piezoelectric, when they are loaded by a mechanical force on the outside, it can create a potential difference (voltage gradient) inside, leading to an increase in hydrostatic pressure, causing the differentiation of mesenchymal stem cells to go through chondrogenesis into the chondrenic lineage. (Dr Brighton also did research in looking at the piezoelectric nature of bone to see how the bone would remodel itself from certain loadings and modifications)
- ESP (Extra Sensory Perception) – I personally don’t believe in too much of this idea and won’t do any research into this topic
- The Body Electric, Electromagnetism and the Foundation of Life (with Gary Selden) – What I would consider his seminal work, especially on what happens when electrical signals is applied to the bone – “He also found that bone has piezoelectric properties which would cause an application of force to generate a healing current, which stimulated growth at stress locations in accordance with Wolff’s law.” – FULL BOOK PDF DOWNLOAD LINK
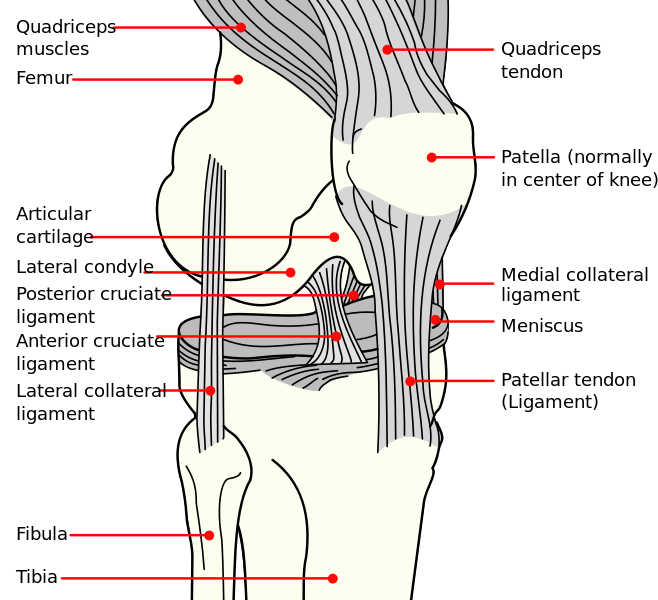
Part #3: The research of Dr. Carl Brighton, specifically his Non-Invasive method to increase growth plate longitudinal growth
The thing I didn’t realize was that Dr. Brighton and Dr. Becker collaborated with each other multiple times, at least in the 70s.
One of the biggest finds in the research was both the scientific study and paper written by Dr. Carl Brighton, a professor of orthopedics at UPenn and one of the lead experts on the growth plate in the world. Dr. Brighton, who I have tried to get in contact with multiple times (only answered me back on the 1st email) wrote up the study…
Study #1: “In vitro epiphyseal-plate growth in various constant electrical fields.” Brighton CT, Cronkey JE, Osterman AL. J Bone Joint Surg Am. 1976 Oct;58(7):971-8. PMID: 185224
Summary: At a voltage gradient of 1500 volts per centimeter, a consistent, highly significant acceleration of growth of the epiphyseal plate occurred… The growth acceleration was due to voltage gradients and not to current flow…. it is obvious that the voltage gradient, either directly or indirectly, incites a physiological response of the growth-plate chondrocyte.
Study #2: “Stimulation of In Vitro Epiphyseal Plate Growth by a Time Varying Electric Field” – Can’t Find the Link to the study
Study #3: “Capacitively coupled electrical stimulation of bovine growth plate chondrocytes grown in pellet form“
Summary: Significantly increased cell proliferation occurred at 500, 750, and 1,000 V peak to peak. The calculated electric fields were 1.5 to 3.0 x 10(-2) V/cm
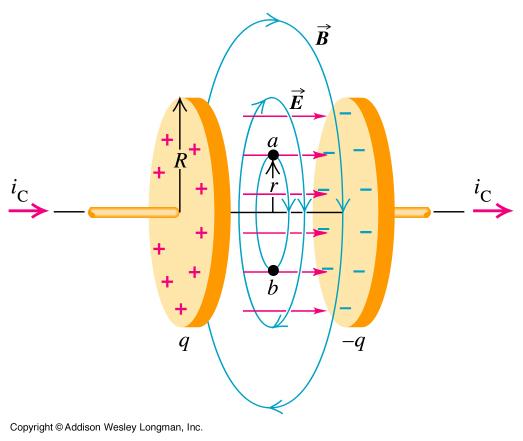 These study was one of the most amazing finds. It showed that if you managed to apply a DC (Direct Current, which is constant) through the epiphyseal growth plate also adding a specific type of dielectric between the two plates, you can increase the bone’s longitudinal growth. It is very similar to what we might see in the Introductory Electromagnetics (E&M) College Course when an engineering student studies on the Capacitative Electrical Fields chapter.
These study was one of the most amazing finds. It showed that if you managed to apply a DC (Direct Current, which is constant) through the epiphyseal growth plate also adding a specific type of dielectric between the two plates, you can increase the bone’s longitudinal growth. It is very similar to what we might see in the Introductory Electromagnetics (E&M) College Course when an engineering student studies on the Capacitative Electrical Fields chapter.
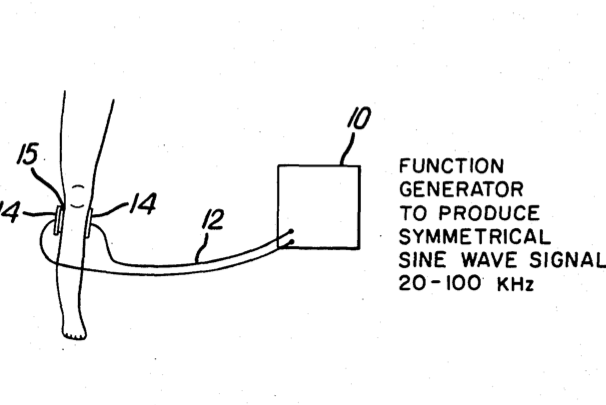 The Patent: Method for non-invasive electrical stimulation of epiphyseal plate growth – US 4467809 A – (1982)
The Patent: Method for non-invasive electrical stimulation of epiphyseal plate growth – US 4467809 A – (1982)
Patent Introduction: Epiphyseal growth plate stimulation in the bone of a living body is achieved by applying electrodes non-invasively to a body and supplying to said electrodes an AC signal in the range of about 2.5 to 15 volts peak-to-peak at a frequency of about 20-100 KHz.
Now, I am aware that the Patent says to use an AC signal, and the studies suggest using a DC for a capacitative electrical field, but the thing to remember is that the devices being sold, the electronic pulse massagers on Amazon are AC since you can change the pulse width, frequency, and intensity.
He also had multiple Patents done in the mid 1980s which solidified that this idea was quite real. They include…
Summary – for the regulation of BMP 2 and 4, TGF-beta 1, 2, and 3, FGF-2, osteocalcin, and alkaline phosphatase mRNA in stem cells via capacitive coupling or inductive coupling of specific and selective electric and/or electromagnetic fields to the bone cells or other tissues containing the stem cells… are useful for the targeted treatment of osteoporosis, osteopenia, osteonecrosis, fresh bone fractures, fractures at risk, nonunion, bone defects, spine fusion, and/or other conditions in which BMP 2 and 4, TGF-beta 1, 2, and 3, FGF-2, osteocalcin, and alkaline phosphatase mRNA and/or protein deficiencies in stem cells has been implicated.
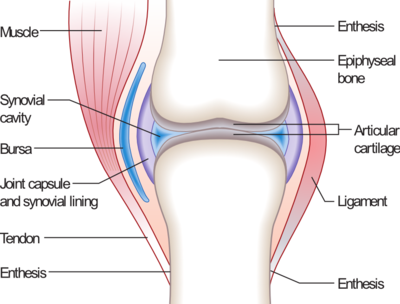
Summary – devices are provided for the targeted treatment of injured or diseased cartilage tissue that include generating specific and selective electric and electromagnetic signals that generate fields optimized for aggrecan gene expression…devices are useful for the targeted treatment of osteoarthritis, rheumatoid arthritis, cartilage injury, and cartilage defects.
Patent #4: Portable electrotherapy device for knee joint maladies – EP 1644074 B1
Summary – selectively up-regulates gene expression of Aggrecan and Type II Collagen while simultaneously selectively down-regulating the gene expression of metalloproteases. The device includes a signal generator that generates compound electric signals including a 60kHz sine wave having a peak to peak voltage of approximately 4.6 V to 7.6 V
The fact is that this Brighton guy has over a few dozen patents he created back in the 80s which are all under his name. The ideas he claimed from the use of capacitatively coupled electrical fields show that cartilage regeneration is possible taking the approach of sending electrical signals of a certain type through to the cartilage areas using this non-invasive method.
He is referenced in the blog Electromagnetic Bioeffects Blog, The blog writes… Sept. 19, 2011 “The 3 B’s and Electrical Stimulation of Bone Growth“ – “…Carl Brighton MD treated patients at the University of Pennsylvania using a method of electrical stimulation in which cathodes were drilled into the fracture site and the return anode was attached to the skin. A company he worked with commercialized the device, and about 80% of the patients treated with it healed in 3 months…developed an electrical method that used magnetic fields produced by two coils attached to the outside of the cast.”
This sound very much like the idea I had about using two coils to produce magnetic field going in a certain direction to pull bones apart (although his idea was to pull bones towards one another) which I wrote about in the post “A Method To Distract Bone Slowly Using Magnetic Fields, Metal Implants, And Acidic Solution“.
Part #4: Comparing this Electrical Pulse Massager to the Low Intensity Pulsed Ultrasound, LIPUS that Tyler has been promoting.
Tyler on his blog HeightQuest.com has been promoting the idea of combining LSJL with LIPUS but I personally feel that ultrasound does not have enough effect on the longitudinal growth. The study “Restoration of longitudinal growth by bioengineered cartilage pellet in physeal injury is not affected by low intensity pulsed ultrasound.” I wrote about the study and its implications in the post “Bioengineered Cartilage Pellets And LIPUS For Longtitudinal Growth (Huge Breakthrough!)” and I had suggest back then that instead of the LIPUS idea, we should go in the PEMF route, since PEMF stands for Pulse Electro-Magnetic Field and that is what Brighton, Becker, and I have all seen from research to work.
Using pulsed electrical fields and signals seem to be a better option than going the Ultrasound path.
Part #5: Connecting all this to Dr. Michael Yessis and a Grow Taller book written by a supposed Soviet Orthopedic Surgeon, a 80s American Physician studying Soviet Bodybuilding Secret, who translated the “School of Height” Book
The book was translated by a Dr. Michael Yessis who turned out to be a very famous well known American Physician who made some startingly discoveries on how to maximize the human body’s potential when he studied how the Soviets trained their olympic athletes also back in the 80s.
It turns out that the book that I got very early on which was given to me by Nikki (Kazlina) had one section which was so unconventional on the idea of taking a certain type of wool or cloth to rub on certain bone areas of the body. The section was very unique and I wondered back then whether the rubbing of wool to stimulate blood circulation was possibly to create a certain type of static electrical charge which might work in remodeling the bones underneath.
If Yessis, who has been a reputable biomechanic for over 30 years was willing to translate this book, the author was probably a real orthopedic surgeon. Why would an orthopedic surgeon put such a strange section like rubbing wool or clothing over one’s knee area unless there was some validity behind the idea?
Everything else in the book was about how to relax the muscles, which would be something the pulse massagers designed for EMS was supposed to do. The person was supposed to do stretching exercises, and try to extend their torso by holding on a bar horizontally. There was a section on autogenic breathing but that was not very helpful.
Conclusion – So What Does This All Mean?
Becker’s research is too vast and large for me to go through right now, and there is already some studies and research which is getting me interested in learning more. Becker’s book The Electric Body has a section in it where he claims that from using a magnetic field, he managed to get salamander limbs to be regenerated at a much higher level.
His study “Electrical stimulation of partial limb regeneration in mammals.” is something I have to go through (don’t have the time right now). Other studies he has done has shown that stem cells can be increased in number through electrical signal stimulation.
Brighton’s work, which is very similar state similar results. If you use an electrical signal of a certain frequency and amplitude, you can cause the upregulation of aggrecan, collagen Type 2, decrease MMPs, increase BMP-2, BMP-7, TGF-Beta2, and a whole host of things. His patents from the 80s reveal a lot of things which validate the idea that the pulse massagers we sell today, seem to have the ability to increase cartilage regeneration, and increase the longitudinal growth from growth plates.
It turns out that if you use the TENS pulse massager devices, the device can actually cause cells to proliferate and divide much more rapidly, as stated by people who have done also a lot of research on TENS.
So when I combined all of the research that these guys did, it suggest that the application of an electrical signal, like that from the few various pulse massagers sold in the market today can indeed increase the growth rate of children, and almost anyone who still has any growth plate cartilage left. At a certain frequency, the growth plates will generate more cartilage extracellular matrix content like proteoglycans and GAG.
Not only that, the control dials on some of these pulse massagers sold can go as high as the values that Brighton claims in his patents. The devices of electrical stimulation he talked about in his patents from the 80s are now in the market today. These devices allow you to control the frequency, and intensity as he suggested. Some allow only the ability to control only the intensity of the signal, but others allow one to change both parameters.
This means that parents can indeed stimulate the growth of their children, make them taller using these pulse massagers, as long as the person still has growth plate cartilage left! What really counts now is finding the best pulse massagers in the market, which operate on TENS and can focus on the exact area.
All that it would take is to put the electrodes of the TENS device which can on the growth plate areas of the leg (or arms) and it should work, as long as the right frequency, and intensity is done. Remember however that the usage must be in a pattern that is called intermittently. Use the device for only 10 minute a day, 2-3 times a week.
I have looked at the selection and the two pulse massagers which seem to have the most promise are…
Device #1: TENS Electronic Pulse Massager Device by HealthmateForever – Price: $90
Device #2: Prospera Electronic Pulse Massager – Price: $32
 Things to understand about how to use these device – The device is powered through battery or by AC Adapter plugged to a wall outlet. It receives AC power but converts it into DC power that gets emitted in pulses.
Things to understand about how to use these device – The device is powered through battery or by AC Adapter plugged to a wall outlet. It receives AC power but converts it into DC power that gets emitted in pulses.
This means that it turns on and off the signal of DC. The frequency is NOT of a AC signal. Remember that electrical signals are sinusoidal in nature since each type of light (IR, X-Ray, Gamma) represent part of the electromagnetic field spectrum.
We have to make sure that we can control the pulsing frequency of the DC signal. – Before anyone buys this thing, make sure that we have the option to not just change the intensity/amplitude of a signal, but the frequency or the speed of the pulsing, since that will be also important.
From Brighton’s research the values for the signal should be an AC signal in the range of about 2.5 to 15 volts peak-to-peak at a frequency of about 20-100 KHz and a 60kHz sine wave having a peak to peak voltage of approximately 4.6 V to 7.6 V to restore articular cartilage in people who have arthritis. These values can definitely be modulated and reached by the current pulse massagers in the market today.
There is a 3rd type of electrical stimulator which might be more accurate in getting the electrical signal to the actual cells in the cartilage of the bone, but I am not sure at this time how it would work, unless we scraped the bones – Pointer Excell II Digital Acupunture & Pressure Point Locator