I wanted to explain where height increase researchers are in terms of development and why it has been so difficult to figure out how to achieve this goal of trying to grow taller after the growth plates in a person have closed.
Many times I have written posts hypothesizing what was the limiting factor or the real problem in figure out a solution to this thing that 99% of visitors to this website is looking for.
I had first tried to explain what exactly was really limiting us as researchers in the post “What Exactly Are The Critical Elements, The Rate Limiting Parts?” In that post, I had suggested that we move away from studying too much on GH (somatropins) or IGF-1 and focus more attention on growth plate formation through using growth factors and chondrocyte differentiation from the progenitor mesenchymal stem cells. At this point, I still agree with this idea.
In another post I had copied a study which showed that no matter what happens, our bodies are designed by evolution to be limited in size. At some point, we will stop growing, if we are reasonably healthy and don’t suffer from certain genetic disorders. The post was “Mechanisms Limiting Body Growth In Mammals“
A few days ago while I was eating dinner with my girlfriend, she started to ask me what exactly I was doing when I spend hours each day doing research and obscure scientific papers. I have not revealed this website and my research to her yet and I want to keep this part of my life hidden. However she persisted and asked me more probing questions about this issue.
(Side Note: Now, I am currently living in Seoul, South Korea and at that moment we were eating this dish at a local eatery which is Pig Feet, known in Korean as Jokbal. While the sound of the idea of eating the feet of pigs may not sound too appetizing to some people who were raised in the western world raised on lean beef, pork chops, and chicken breast, it turns out that it is really good and surprisingly good for a person who believes in the Paleo Diet.)
I glanced at the food in front of us, which was just meat bones and I managed to come up with a very simple explanation of what it was that I was doing without revealing her the entire scope of the research.
I picked up a leg bone of the meat in front of us and showed her that in the limbs of mammals, there is two types of structural tissues, bones and cartilage. She understood that much.
I then said that all that my research is trying to do is to try to convert bone tissue into cartilage tissue. That is what I have been trying to do.
I indicated that what I was trying to do was create a band of cartilage through the entire cross section of the long bone.
Bone Tissue —> Cartilage Tissue
From this simple concept is how the entire height increase endeavor can be summed up. Now, the way that the natural process works is the reverse process. Cartilage Tissue into Bone Tissue.
Cartilage Tissue —> Bone Tissue
If one would like to read on why and how cartilage tissue turns into bone tissue, I refer to the PubMed study “Cartilage begets bone versus endochondral myelopoiesis“. Analogously, cartilage tissue, at least hyaline cartilage, is almost always surrounded by a layer of progenitor cells that have not differentiated yet called perichondrium. In the same way, bone tissue at least in long bones are surrounded by a bilayer of cells known as periosteum.
The process that happens in nature is perichondrium turns into periosteum.
What we are trying to do is create a simple, non expensive way to start a process that is exactly the opposite or reverse process of a natural process.
- Bone Tissue —> Cartilage Tissue (going against nature)
- Cartilage Tissue —> Bone Tissue (how nature works)
To grow taller, we can do only four things that I can think of currently. We are either…
- Stretch the bone tissue
- Implant something into the bone tissue that can stretch out
- Implant a device in cavities between bones that determine height
- Turn the bone tissue, at least part of the bone tissue, into cartilage tissue
Option #1: Stretch the bone tissue
First, I had looked into the idea of just how feasible was the idea of just getting some weights or some traction device to stretch out one of the bones in our body to make us taller.
Since human height is determined by the following bones in the human body… skull bone, the vertebrate bones, from cervical to the coccyx, the hip/pelvic bone, the femur, patella, and tibia/ulna, and talus with calcaneus… these are the only bones that we need to worry about.
I would assume that no one would want to stretch out their skulls so that it out of the question. For the vertebrate bones, that is reasonable but the bones are irregular, and if we try to pull the bones too hard, we can cause serious problems to the surround tissues, most specifically causing intervertebral disc problems like bulging discs or herniated discs. Given just how common herniated discs and lower back pain is to humans, I am currently not going to pursue the idea of trying to stretch out the irregular vertebrate bones just for cosmetic reasons.
This leaves just the idea that maybe we can figure out how to stretch out vertically the pelvic/hip bone, the leg bones, or bones in the feet. Since the pelvic bone and feet bones are irregular, it might not be very feasible to stretch the bones even in a laboratory setting. How would the pelvic bone even be held by a mechanical device to stretch it out?
So the only bones that are left that have any possibility of being stretched comes back to the long bones.
I tried to do a rough calculation of just how much loading must be done to the adult human femur to pull it beyond the range of elasticity and lead to some form of deformation.
The post where the real calculations were done on was…
The Values For The Magnitudes For The Forces And Loads Needed To Increase Epiphyseal Cartilages Thickness And Human Femur Bone Without Fracture (Important)
From taking the measurements of forces done from tensile loading on the cartilage of young lab rabbits, I did two extrapolations calculations to reach the answer that to stretch out the human long bone in the legs, specifically the thickness, strongest one, the femur, it would take between 29,000-32,000 lb of force to pull the adult human’s long bone apart.
My calculations seem to be actually reasonable close to what was guessed to be the needed tensile values of human bone by other researchers who did real experiments with the leg bones of cows. Their proposed values for ultimate yield strength of human femur bones was 150 MPA (Mega Pascals) which when converted into the American unit of force, the pound-force, or pound, is 22,000 lbs. For certain engineers, getting a final calculated value within even 50% to what it is supposed to be is good and I am guessing that the values between mine and other researchers are close enough to start to support the idea that a tremendous amount of force is needed to pull the strongest bone in the human body beyond it’s ultimate yield strength point.
Years ago there was another serious height increase seeker and researcher named Sky who tried to induce height increase their hanging weights on his ankels to try to lengthen the tibia with 15-30 lb weights on each leg. He did not succeed. The rough calculations shows that his method would not have worked. He would have needed to use weights that were 100X in weight to have a chance of pulling the tibia bone apart.
Important Note: The way that the tensile loadings work is that successively smalls increment of weight is added over time to the material being tested. If we instead tried a type of loading that was not slow and linearly increased, like a fast jerk, it might be possible that it would take less weight and force to cause the bone to snap or fracture into a lengthened state.
If the calculated values are correct, which involves the unit of lbs in the 5 digits, then where would the average person with limited resources even be able to find devices that can product a stretching/tensile load that high?
Even regular sized 4-door sedans are only around 4,000 lbs. Adult bull African Elephants, the largest land animals in the world are at 8000-10,000 lbs only. It might be interesting to imagine holding one part of the long bones in the leg in place and having a weigh attached and have a 3 full sized elephants or 6 cars get on on the scale.
What type of device can the average person get their hands on to generate that much force? I don’t know whether there are any mechanical devices that can do that without also being associated with a very high risk for severe injuries that would lead to a person being crippled for life.
Some people talk about using electrical field or magnetic fields to pull the bone apart. An idea that was recently talked about was using an induced magnetic field to pull two metal implants further apart in the post “A Method To Distract Bone Slowly Using Magnetic Fields, Metal Implants, And Acidic Solution”. I personally only gave a general idea on how it might work. Much more research would have to be done to see how reasonable lengthening bone using electromagnetic fields are.
Even if it was possible to get a device that can generate that type of force, there is an extremely high chance that instead of experiencing plastic deformation by the bone the bone due to how brittle it is, would just fracture and snap in two pieces. Remember that the calculated value was for the Ultimate Yield Strength for the bone from looking at it in a Material Sciences perspective.
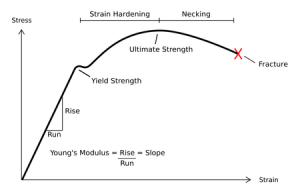
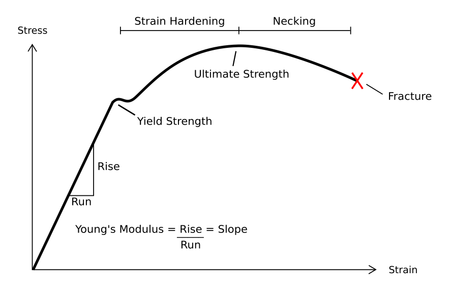
In the post “The Concept Of Youngs Modulus, Stress, And Strain Explained For The Application Of Bone Tensile Loading Or Bone Stretching (Important)” we looked at the engineering terms of young’s modulus, yield strength, ultimate yield strength, and other terms to explain just how “brittle”, elastic, and deformable was the human bone.
 We know that in general the human bone is brittle, especially when it is taken out of the body, and left in normal air conditions which lead to the bone lossing water, dehydrating it, causing it to loss whatever little elasticity it did have.
We know that in general the human bone is brittle, especially when it is taken out of the body, and left in normal air conditions which lead to the bone lossing water, dehydrating it, causing it to loss whatever little elasticity it did have.
Note that the picture to the right is one of the general stress-strain graph of materials.
From an in vitro perspective, human bones are too brittle to have a large enough range of strain values to be able to get to what can be called the perfect strain region. We know that if the amount of strain is increased to a point which is below the yield strength, it will just snap back in place since bones are technically elastic, but it is just that the deformation in terms of length from a tensile load is almost negligible. If the amount of loading is increase too far, it would go past the ultimate yield strength, and the bone would fracture, and fracture so badly that the person basically pulled their leg off.
While the graph to the right is very general and is used as a diagram to show how the stress-strain relationship really works, because the bones are so brittle, there should be almost no range for the material science term called “necking”. Not only that, the range between yield strength and ultimate yield strength might be so small, that the yield strength is the ultimate strength. What if there is no range for a tensile load which would get the bone to the plastic deformation and not to the range where major fracturing would occur.
Option #2: Implant something into the bone tissue that can stretch out
I had made a note of the idea that maybe the biggest problem is not the bones themselves, but the surrounding tissue, the muscle that is causing most of the difficulties in the post “The Rate Limiting Tissue May Be The Surrounding Muscle, Not The Bone”.
The one of the most common difficulties with replying to people who wish to increase their height as adults is that they state that they are willing to try almost any idea except go through with the option of surgery, specifically the limb lengthening surgery.
I had expressed and ruminated about the issue of the need to always distract bone to increase height superficially in the post “Is Bone Distraction Or Bone Breaking Always Needed To Increase Height?“
Anything involving an implant would most likely be invasive, and that means that the person can no longer do the needed steps in the privacy and comfort of their homes, away from the public judgement of other people. The desire to not reveal who they are is a very big concern for people who try to increase their height. Most people I ask to come on the podcast and speak say no. They are afraid of the social repercussions of the possibility that someone that they know would hear their voice and reveal this side of themselves.
One could say that maybe it would just be smarter to implant newly grown or explant growth plate/cartilage into the bone, but that would still require that a section of the bone broken apart. If that is the option that a person would suggest, maybe it would be smarter, and less invasive to figure out whether we can turn the bone tissue already there into cartilage tissue. That option, option #4 is the one that I and other researchers would like to figure out.
Option #3: Implant a device in non bone cavities between bones that determine height
This idea is actually a little more credible than some people might believe.
I did a recent post about this idea when a regular reader showed me this revolutionary surgical procedure where a titanium stent is implanted into this cavity in the feet of human which is made of only ligaments, with no bone tissue. The post was “Do People Get Taller From Flat Foot Corrective Surgery With A Hyprocure Implant?”
It seems that there was a guy who wrote a blog talking about how his condition of flat feet made him decide to get a feet implant to decrease pain in his legs and back. As a result of the surgery, he noticed that he became half an inch taller.
So what other cavities that are between bones can we theoretically implant something to make ourselves taller?
The first thing to realize is that for most cavities between bones, they are filled with some other type of tissue, like ligament, cartilage, or extracellular fluid (like the cerebral spinal fluid)
The most obvious location would be the synovial joint of the knees. However, I am not sure how many people who wish to become taller would be willing to implant any type of metal into their knees just to be a few cms taller. I know that there is a chance that getting some aggrecan or hyaluronan injections into the synovial cavity may lead to less diurnal variation as the day goes on but I am not aware whether there is any type of device that any researchers have been doing to get height increase their knee implants.
If we try to find other joints or cavities which can be expanded, I am left to wonder maybe it is reasonable to try to hypertrophize and expand the thickness of the intervertebral disks. Technically, the disks are cavities between the vertebrate bones since the definition I am using is that the term cavity implies any space between bones that determine the overall height that is not consisting of any bone tissue. The disks are made from different types of collagen and some cartilage so they are ‘cavities’ as defined for this unique application.
This is actually the idea that most people have on how to explain why using traction, inversion machines, stretching, yoga, rolfing, all lead to permanent or temporary height. You are NOT stretching out bones, but stretching the cavity/non-bone tissue that contribute to the determination of one’s height.
Option #4: Turn the bone tissue, at least part of the bone tissue, into cartilage tissue
So if we don’t like the idea of breaking the bones through surgery to get at least the initial distraction, if we can’t get the type of machinery or device to exert upwards of 30,000 lbs of tensile force, and if we have no cavities that we would be willing to accept to get metal or plastic implanted into our body, then the last thing is to try out is whether we can turn the bone tissue that is in our body into cartilage tissue.
Remember, all that I have really stated is that to expand volumetrically a very tough, hard object that is not very elastic and brittle, there is only 4 things that we can do try out.
- Use brute force with pliers and pull the ends of the tough material and hope that it does go through with plastic deformation with completely fracturing and breaking in half.
- Put a cut, laceration, distraction, fracture, or a physical break in the object and then stretch it using the same devices we would use in the first option. This idea would involve the actual object being broken but the amount of force needed to pull it apart to expand the overall structure’s size volumetrically decreases dramatically.
- If there are any spaces within the object which is not already filled by the material, put something in the space that can push out the object around it and potentially make it bigger.
- Turn a part of the material into a another type of material with completely different material properties. With our intended situation, we want to make the bones turn into some other material that can still be strong enough to hold up a person who can be over 200 lbs but also have the plastic elasticity needed to be pulled/expanded using a reasonable amount of needed tensile load.
I hope as researchers we never forget that the reason the extremely hard bones can even lengthen at all in the first place is because in the beginning, the tissue was not bone, which is extremely hard and brittle. In the beginning, the type of tissue was cartilage, hyaline cartilage.
It is hyaline cartilage which has the right type of mechanical qualities which makes it possible for humans to even go through a type of somatic growth as vertical growth. The entire process of endochondral ossification revolves around cartilage tissue, NOT bone tissue, although the end result or output of the endochondral ossification is bone tissue.
It is cartilage that is between two parts of bone tissue which get expanded out due to the fact that the microscopic cells in the cartilage extracellular matrix tissue (the chondrocytes) start to actually expand in volumetric size, and by doing this, they push the entire matrix and the entire matrix gets bigger, like a loaf of bread that gets baked in the oven.
When the chondrocytes hypertrophize, while the effect for themselves is get bigger by maybe 5 X, the effect the cells have on the tissue outside the outer cell membrane is that the organic and inorganic composition that forms the matrix gets pushed farther apart from each other. If we used a microscope to do a histological examination, and we took pictures of a set of points (A, B, C) and then noted the distance between those points, and then noted the distances between the same points but now after the chondrocytes have hypertrophied (A’, B’, C’) we would realize that the 2nd measurements on average would have gotten bigger apart. The main point is that when the cells in the cartilage matrix expand/ or puff out, they puff out the entire cartilage.
(Another good analogy is the idea that as the distance between the galaxies get farther and farther apart, we can say that technically the size of the known universe, as defined as all the space that the galaxies can reach, is get bigger)
This means that the entire ability of bones to get longer is from cartilage tissue.
Technically, it might be possible to lengthen bone if the cells of bone, the osteon, the osteophytes, and osteoblasts could go through their own type of hypertrophy where they expand out and get bigger, but there does not seem to be any way for them to do that, at least not that I known of.
This shows that maybe the easiest option in terms of simplicity of concept theoretically is the last one, where we just replace the bone tissue to cartilage tissue, but also possibly the hardest option to actually execute and implement correctly.
- We know that physicians can land have increased the length of long bones using the 2nd option, where a break in the bone is done in the beginning, so that the external device can actually pull the bone apart.
- From the Hyprocure Stem Implant, we know that the 3rd option has also been done and is also successful in giving a small amount of increased height.
- I and other researchers have seen that that many height increase seekers and researchers have tried the 1st option, what I call the brute force method, and none of them have succeeded. I propose now that the reason that the idea of just stretching a bone does not work is because the amount of force needed is much, MUCH more than what was used before.
In some ways, we can view endochondral ossification as an internal process that causes the cells in the bone-cartilage matrix to push the entire structure outward. The cells inside the cartilage is pushing the tissue outward from the inside. It might be that maybe we can figure something out that can get the bone cells, the osteoblasts to expand outward in a specific direction, and get into a columnar formation.
Now, I am fully aware that for people who wish to grow taller, then want something easy, simple, cheap and something that they can implement and do alone in their homes without other people finding out. This means that for most people, the idea of breaking the bone is rejected almost by all seekers. So distraction of even a section of the bone is something people refuse to consider.
Surgery for most people is just out of the question. They are willing to try anything else, just not surgery. I completely understand this way of thinking and sympathize with everyone since it is generally accepted that the surgery that does lengthen bone is very expensive and painful.
Everyone wants something non-invasive and wish for a magic chemical compound that they can swallow. I wrote about this problem in the post “There Is No Magic Bullet”. The fact that nearly everyone wanting something that is non-invasive or minimally invasive makes the situation extremely hard.
Even with the case where scientists and researchers can regrow a completely functional growth plate, many people still will not accept this approach because to get the new growth plates, their limbs will still need to be operated on to get the growth plate cartilage implanted into the bone and that would involve distraction still.
This shows just how difficult our searching and research are. Due to how people want certain things in certain ways, and refuse all other options, it seems that even with a breakthrough like showing that functional growth plates have been already been grown in vitro, which I had wrote about in the past “Engineering Growing Cartilage Tissue In Vivo Through Chondrocyte Transplantation (Big Breakthrough!)”, people will still be searching for something better because they are still not satisfied.
I am reminded of a conversation I had with a superior at a company I had interned at during the summer after my sophomore year in university. The company’s goal was to develop a way to disrupt the normal viral vector- cell membrane process that occurs in AIDS. They were trying to cure AIDS. At the time, the only way that the scientists could figure out how to deliver the drug was through it getting released into the blood stream through a needle injections.
My superior made the side remark that if a competitor company who was also trying to figure out the right release patterns of dispersion for the same compound could create an oral version, none needle version of this treatment, the company would get destroyed. The conversation showed me that when it comes to medical treatment or any type of cure to solve a problem, people want something easy, something that doesn’t require any type of work. For humans, swallowing a pill to cure AIDS for them was a much better option that getting a syringe-needle subcutaneous injection to cure AIDS. People wanted the best, easiest option for themselves. In the process, I feel like too many people try too hard in emailing me asking me for some magic or secret technique or formula to help them grow taller.
At this point, I could send an email reply telling a person to ingest mercury (Hg) at 5 mg per day to grow taller, and some people just might be willing and actually do carry through with it to get it.
WARNING: The previous suggestion is something that WILL NOT WORK. I was just using the idea as an example of a crazy suggestion/reply to people’s emails, which people might think was the ‘magic secret’ which would make them increase in the 9-10 inches that they want. Well it won’t work. Don’t swallow mercury.
At this point, I would think that to really satisfy the people’s desires, we have only two options.
- We figure out how to get a band of bone tissue in the long bone to turn into cartilage.
- We try to figure out whether we can get bone cells, osteoblasts and osteocysts (or whatever other living cells in the bone matrix) to hypertrophize like the chondroctyes in growth plate cartilage.
Option #1: We figure out how to get a band of bone tissue in the long bone to turn into cartilage.
The first idea would be the one that could be more likely to work out. I think that at this stage, the limiting step or weakest link of our research is figuring out just how to get the bone tissue to turning to cartilage tissue. Again, remember…
Bone Tissue —> Cartilage Tissue
As long as we can get the bones to turn into cartilage, I am going to propose that everything after that should be relatively easy.
I realize that maybe the easiest type of cartilage to form would be the fibrocartilage, the type of cartilage that is formed when one drilled through the subchondral layer of bones, and hit the marrow in the intermedullary cavity, which will start to spurt/leak out and then the mesenchyme in the marrow start to differentiate into cartilage, but a type that is not as strong or good as the hyaline cartilage that we really want.
However, I suggest that we first just figure out how to go from bone tissue to fibrocartilage first, and then try ot figure out how to go from fibrocartilage to the better hyaline cartilage.
The second thing to figure out if we do manage to turn bone into cartilage, is how to get enough chondrocytes in the cartilage to start to proliferate. However, I say that this step should be relatively easy by just taking some explanted chondrocytes and using a syringe injecting them into the cartilage.
To get the chondrocytes that are injected to start to proliferate , we just add a growth factor mixture, something like BMP-7 with TGF-Beta1-3 through another injection.
The last big thing to work out once we do get the chondrocytes to start proliferating is how to get the chondrocytes to start to get in the right alignement, to form the columnar formation which allows to actually push the cartilage longitudinally. However it turns out that we have discovered that the compound Thyroxine seems to cause the chondrocytes in the natural growth plates to get into the right direction/orientation for long bone longitudinal growth. This was talked about in the post “Thyroxine Regulates The Morphogenesis Of Isolated Chondrocytes Into Columnar Cartilage (Big Breakthrough)”
At this point, I suspect that the process of chondrocyte hypertrophy is almost always automatic after the chondrocyte reach the later stages of life when they are ready to go through apoptosis.
I also am going to assume that the tissue interface between cartilage and bone will always be continuous and should run smoothly in causing cartilage to vascularize and mineralize.
This is why I am saying that after we get the right compound added to the converted cartilage tissue to get the chondrocytes implanted inside to align into columns, the rest can take care of itself. (However I could be wrong about the assumption on the cartilage-bone interface and the fact that chondrocytes will always go through a hypertrophy stage releasing alkaline phosphatase)
Option #2: We try to figure out whether we can get bone cells, osteoblasts and osteocysts (or whatever other living cells in the bone matrix) to hypertrophize like the chondroctyes in growth plate cartilage.
The truth is that this idea of trying to make the bone cells in the cortical bone and trabecular bone of our limbs to start to expand in size, just like what the chondrocytes in growth plates do is something that I just proposed today.
After finding the studies by much researchers do did mechanical tensile loading testing on cow leg bones from 100 years ago stating that the amount of force to actually pull a long bone is around 30,000 LBs, I started to move away from the idea of ever being able to lengthen boen using brute force.
I personally don’t have a robot or device that can pull in opposite directions with over 30,000 of force in a very linear increasing fashion. I also don’t want to risk the possibility that if the loading of such a force gets increased too fast, my leg might snap in half and I become crippled for life, or even loss a leg or limb.
This means that if the height increase seeker wants to really find a non-invasive or minimal invasive approach, they are going to need somehow turn on the components that are already in the bone matrix to start to puff themselves up and possibly increase the bone size.
They will have to stimulate what is inside and get that to push outwards, instead of trying to use mechanical, electrical, or chemical devices and which will apply stimuli externally.
At this point, I am not even sure how to get started on this type of research yet, since the idea came only today.
I am aware that there are some types of bone cells that do get bigger and go through hyperplasia, but I have always associated it with metastatic tumors that get out of control or the formation of bone spurs on the surface of bones by osteoblasts that start to proliferate and hypertrophize too much in the adult human.
Now, I and the other researchers are quite aware that even if we can get the bone cells to start to expand, the cortical bone matrix with the calcium minerals embedded might be very resistant from expanding like cartilage matrix, which is much softer and elastic.
This is why I am proposing two idea on how to ‘soften’ the bones to a point where maybe the targeted bone region can be softer than the surrounding bone tissue.
1. Adding Ascetic Acid/ Vinegar/ A Weak Acid
Adding a weak acid to remove the calcium apoxyapatite which might be similar to a normal acid-bad reaction which neutralizes the targeted area. I wrote a post about the fact that if you put bones and put them a few days in vinegar (composed of ascetic acid), the calcium minerals that make bones hard get removed, leaving just the collagen, and the bone as a result turn into rubber, and that bone tissue can definitely be stretched out.
The post was “Using Acids To Induce Reverse Ossification For Calcium Mineral Absorption”
2. Adding PTHrP/ PTH in the right dosage to turn the bone such soft enough while having enough strength to keep the integrity of the overall boen structure intact.
In one of the most important posts I have written, I showed that the compound PTHrP would be critical in causing chondrocytes to not completely differentiate, reverse differentiate, and can be used in combination with growth factors and other compounds to generate cartilage and demineralize the bone matrix, making the overall thing softer and more malleable.
The post was “Parathyroid Hormone And Parathyroid Hormone-Related Protein May Lead To Non-Invasive Epiphyseal Growth Plate Regeneration (Big Breakthrough)”
The other post that was the original source is “The Connection Between Regenerating Deer Antlers and The PTHrP, PTH And IHH pathway for Cartilage Regulation, PTHrP Seems To Be The Answer (Big Breakthrough!)”
So it seems that the other idea, which I am not sure how feasible, is to get the bone cells to expand and push themselves against the bone matrix and lacunae and possibly get the bone to increase volumetrically.
Overall Conclusion
The thing to realize is that what we want and what is even theoretically possible does not agree with each other. There really is not a lot of options to the individual.
What the average person would love to do is just swallow some strange chemical concoction and end up taller within a few months but that just won’t happen, at least for people with closed growth plate.
Everyone who messages me want something easy and cheap that they can do in the privacy of their own homes.
I look at something like the Lateral Synovial Joint Loading technique that Tyler who writes for HeightQuest.com has been proposing for over 5 years now and I would say that it definitely would be the best, most clever idea for a “height increase hack” I’ve seen so far.
There is some evidence that it might work and there is also evidence that says that it won’t work, that the experiments done on rats can not be transferred and applied in the same way to the human body.
Beyond what the LSJL can offer, Someone recently sent an email to me asking whether I knew if “there’s something more potent that the guy at home can do?” I say NO.
HOWEVER, there might be something that can be done along with LSJL which can greatly increased the chances of it possibly working. What might help with the lateral loading was this idea I had proposed where a person can remove tension from the covering of the bone to let the germinal layer of the periosteum to potentially turn into the chondrogenic lineage and push out/ elevating the entire bone structure just slightly.
I wrote about the original idea in the post “An Alternative Explanation On Why The LSJL May Actually Help People With Closed Growth Plate Increase Height And Grow Taller (Big Breakthrough!)”
The idea of using another instrument, a hammer and chisel, to cause a tear in the periosteum to decrease bone layer tension to increase the chances of LSJL was expanded a lot more through the video post “The Chisel And Hammer Supplement Technique Explained Through Video”
For The Future
There is nothing we can do to get around this thing, at least right now. The research will focus almost exclusively on learning more about how the underlying mechanism for somatic work is currently understood. That involves a lot of research on endocrinology.
Interestingly, I recently started to learn much more about anatomy, physiology and pathology and tried to take a USMLE Step 1 Practice test just for fun. Out of the 322 total problems on the test (46 questions for each section with 7 total sections), I got only around 60 questions right, and that was sad since it was a multiple choice exam with at maximum 5 possible choices for each question (sometimes 4 options). If I had just chosen A for all of the questions, theoretically I should have gotten around 64 questions right. Note that to pass the USMLE Step 1, a person needs to have a score of 188 or better, the average pass rate is around 97%, the national average is around 220-225, and that to get into the most competitive fields like Radiological Oncology or Plastic Surgery, one needs to get a score around 243-249.
(Side Note: For the potential physician, a good resource from the National Resident Matching Program to see just how well they need to perform on these standardized tests to get matching for the speciality that would like to focus on in their medical career is located HERE.)
I don’t plan to ever be a physician any time soon since I find the field of medicine rather boring. However, I do read up a lot more on medicine and biology as well as genetics these days, unlike my undergraduate days when I hated anything related to biology.
I understand that at this time my knowledge on the human body and its numerous ways to go bad is severely limited compared to well trained medical school students.
There is no way to see into the future. I know that the idea of using stem cells combined with tissue engineering can lead to a alternative to limb lengthening surgery to lead to height increase in adult humans. That approach would definitely work but it is important for the seeker to remember to get something like an implant of a new growth plate to start growing again, they would still need to go to the hospital, talk with a surgeon, and get some type of surgery, which would be invasive. Is that okay for humans or would they want something better, because maybe we just can’t figure out something better.
Side Note: After doing the research for over 1 year, it turns out that there is at least a dozen methods and ideas which would help adolescents and children with open growth plates to increase their somatic growth which are mostly inexpensive, not too time intensive, and non invasive. There is definitely A LOT of hope, options, and chances for children to increase their growth rate and final adult height if they (or their parents) want to make themselves taller. I do plan within the next 2 years to write s seminal work on describing just what is possible for people with open growth plates from analyzing the real science of growth.

{kind=link}