
How Pregnancy Women With Ossified Epiphyseal Cartilage Increase In Height
 For almost a year now, we’ve been getting a few comments made by females which suggest that they seemed to have gained anywhere from 1-3.5 Inches in height after pregnancies or multiple pregnancies. The phenomena is something that occurs usually on the first pregnancy, but sometimes the greatest change is seen on the 2nd pregnancy. The range of ages for the women that have posted on the various internet forums have been from 24-34. The one common factor is that they all had gone through with pregnancy, or were going through pregnancy at the time.
For almost a year now, we’ve been getting a few comments made by females which suggest that they seemed to have gained anywhere from 1-3.5 Inches in height after pregnancies or multiple pregnancies. The phenomena is something that occurs usually on the first pregnancy, but sometimes the greatest change is seen on the 2nd pregnancy. The range of ages for the women that have posted on the various internet forums have been from 24-34. The one common factor is that they all had gone through with pregnancy, or were going through pregnancy at the time.
The fact is that this phenomena is something that was noticed before by other researchers of height increase in adults. The person who created the website www.HeightEffects.com who called himself Height FX back in 2011 asked on a Mommy Forum about the phenomena trying to get more information. He definitely did his research and knew his stuff, but he never got any answer back from any of the mothers about this most unique of phenomena.
His formulation to help young kids with open growth plates to grow was spot on, with his 4 fold-explanation on how his ‘grow taller pills’ were scientifically validated. The 4 methods he mentions are…
- Anti-Fusion Complex
- Androgen Optimizing
- Somatotropic Signaling
- Intracrine Augmenting
In the end, he probably realized that reading another hundred PubMed studies on the mechanism of bone growth, cartilages, and chondrocytes would not be enough. Have a good understanding on the molecular mechanism of human growth and reorganizing the information for easy understanding to validate an internet product (which has the extracts diluted too low to have any effect) is not enough. The science made sense, and it was presented clearly though.
It does not work since there is not going to be some type of PubMed study which would have that type of information. If such a study existed, the researcher would have become a multi-billionaire marketing that method, technique, or idea to Venture Capitalists. He looked for more but never found that.
Refer to our review on the guy and his research in the post “Review Of HeightFX From The Old Height Effects Website”
This entire phenomena is something that we found out about a year ago, but we have not had a lot of time to focus on that path in research. We suspect that this phenomena is much more common than believed, but it is either just not noticed or not reported. Personally, if we were pregnant women, the last thing we would be focusing on is our height. There would be too many things we would be focused on and worrying about. It makes perfectly sense for this type of phenomena to be reported in so few numbers.
Refer to our older posts….
- Analysis On The Possible Cause For Height Increase During Pregnancy
- Another Case Of Pregnancy Causing Woman To Grow Taller And Increase In Height
- More Evidence That Pregnancy Can Increase Height, WOW!
Recently some new information have come in which can explain why a select few women have experienced this most unique of experiences.
If we remember back to our courses in high school about human sexuality and development during puberty, we are reminded of a very unique fact, which is that the hips of the females are supposed to get wider as they are going through puberty. If the hips are getting wider, is it the tissue/fat around the hips that are accumulating, or is the pelvic bone actually becoming wider?
If it is the latter, then how does the physiological process actually work out? How does the pelvic bone wing/iliac crest in the female during puberty get wider?
I was looking for stories & studies about the effects of estrogen on the role of the hip bone, and there were a few women who came forward to state that taking estrogen pills does seem to result in wider hips. That would then explain the connection between wider pelvic bones in women and the increased release of estrogen/female hormone into the system. However, since estrogen is supposed to be increase in puberty for both males an females, then the hips of men should also increase in width shouldn’t it? That is one of the conflicting points of our analysis.
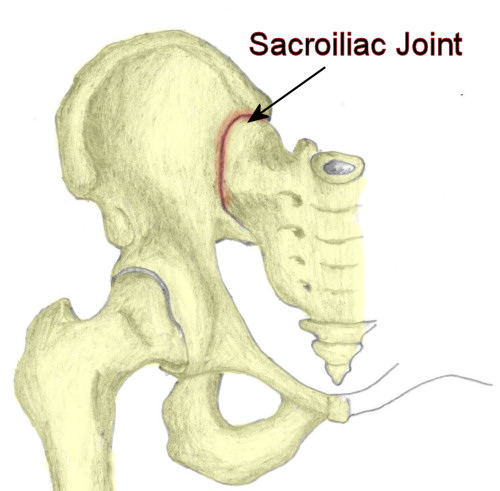 If we look at the way that the entire pelvic girdle area is aligned, we see that the iliac sides are connected to the sacral bone through cartilage types at the sacro-iliac joint, which is in the center region, and they are connected to each other on the anterior (front side) by the symphysis pubis. The Symphysis Pubis is a “….fibrocartilage joint which may contain a fluid filled cavity and is avascular (has no blood vessels) ; it is supported by the superior arcuate ligaments…”
If we look at the way that the entire pelvic girdle area is aligned, we see that the iliac sides are connected to the sacral bone through cartilage types at the sacro-iliac joint, which is in the center region, and they are connected to each other on the anterior (front side) by the symphysis pubis. The Symphysis Pubis is a “….fibrocartilage joint which may contain a fluid filled cavity and is avascular (has no blood vessels) ; it is supported by the superior arcuate ligaments…”
Note this interesting fact: In normal adults it can be moved roughly 2 mm and with 1 degree rotation. This increases for women at the time of childbirth!!
As for the sacroiliac joint, since it is a joint, there are two surfaces of bones covered in cartilage touching each other. You have fibrocartilage-type cartilage on the iliac crest bone surface positioned in the medial direction. You have hyaline cartilage type on the sacral bone surface pointing laterally.
Refer to the studies…
- Sacral and iliac articular cartilage thickness and cellularity: relationship to subchondral bone end‐plate thickness and cancellous bone density
- Variations in thickness of articular cartilage in the human sacroiliac joint.
- Age-related changes in the articular cartilage of human sacroiliac joint
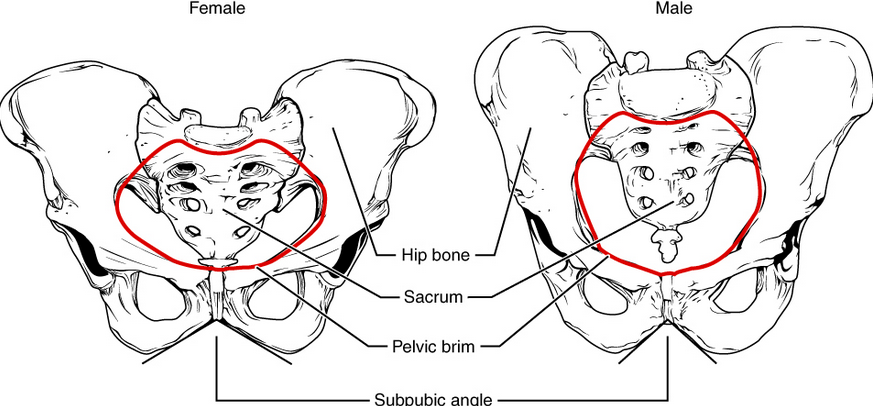
Notice from the picture above how the overall pelvic structure, of the female is wider and thinner in thickness compares to the male’s.
It turns out that one of the most common medical problems experienced by women during pregnancy is lower back pain. Often the blame is given to a condition known as pelvic girdle pain.
 That was the beginning of our research. From the Wikipedia article on pelvic girdle pain…
That was the beginning of our research. From the Wikipedia article on pelvic girdle pain…
…..Pregnancy begins the physiological changes through a pattern of hormonal secretion and signal transduction thus initiating the remodelling of soft tissues, cartilage and ligaments. Over time, the ligaments could be stretched either by injury or excess strain and in turn may cause PGP…..A combination of postural changes, the growing baby, unstable pelvic joints under the influence of pregnancy hormones and changes in the centre of gravity can all add to the varying degrees of pain or discomfort…”
There is also a very common related medical condition known as diastasis symphysis pubis, which is where there is no fracture, but pubis bones are disconnected. From the Wikipedia article, we quote the following excerpt…
“…pregnancy hormonal influences cause relaxation of the connecting ligaments and the bones separate up to 9 mm. To demonstrate instability of the joint the patient is required to stand in the “flamingo” position, (standing with weight on one leg and the other bent). A vertical displacement of more than 1 cm is an indicator of symphysis pubis instability.A displacement of more than 2 cm usually indicates involvement of the sacroiliac joints”
So the ligaments separate. During normal pregnancy, the separation is around 4-5 mm, but with this certain condition, the separation increases to around 9-10 mm. If the separation is up to 20 mm, then then the effect is no longer in the pubis region, but is also affect the two other joints, the sacroiliac joints in the back.
This explains the idea that during pregnancy, the ligaments holding the three joints which normally hold the entire pelvic region in place making it immobilized, becomes lossened.
We are guessing that the looseneed ligaments around the three joints actually makes the joints expand out, making them almost double jointed in nature. The entire pelvic region can be expanded out. This is for easier passage of the baby through the birth canal, during labor contractions and labor pains.
When we consider the fact that once the joints are expanded, the angle of the iliac crest being positioned to the sacral bone is lowered. If the iliac crest is pulled down by an angle, the hip socket which is part of the bone is also lower. Since the hip joint is lowered, the entire lower limbs/legs become positioned farther away from the torso of the body. This translates to an increase in height.
Sometimes we forget that the overall height of the human is more than just the legs and the spine. There is also the cervical vertebrate or neck, the head, the hips/pelvic bones, and the feet. We can modulate and stimulate anywhere as long as it is safe for the person going through with it.
The Other Possibility
When we first reported this phenomena, Tyler proposed that the most likely explanation is from a chemical/hormonal compound. Just one compound, Relaxin. Refer to the post “The Connection Between Relaxin And Possible Height Increase“
At this point, I am almost positive that Relaxin may be the chemical compound that causes the initial loosening of the ligaments, but the actual morphological change in the structure of the bones is what I propose above, which is where the sacroiliac joint loosen by a certain angle, causing the hips to become wider and the iliac crest to drop lower at the same time during pregnancy.
This idea that the hips get wider is validated by this Yahoo Questions we found “Does your hips get wider during pregnancy?”. One of the people who answers understood the importance of relaxin.
There are enough anecdotal stories and evidence of women who stated that after their first pregnancy, no matter how much they exercised their gluts/buttocks and core muscles, they could never decrease their hip size back down to the length of before ever being pregnant. This sort of indicates that the the problem is not muscle tissue or adipose tissue, since you can mold those through exercise. With bones, you can/t The hypothesis is that their hips or overall pelvic bone structure changed.
This type of change would be enough to explain maybe 1 inch of noticeable change in height, but how would we explain away something as large as 2 inches of increase? At this point, we can only propose that it is a combination of multiple physiological processes.
Process #1
You have the increase in feet size from pregnancy, which has been validated by maybe 10-15% of all women who went through pregnancy. A quick discussion among new mothers will bring up the fact that their old shoes don’t fit. Their feet not only got wider, but also longer. How does the bones in feet make it longer? It can’t just be from the ligaments from loosening, although we are sure that the ligaments loosening is part of it. Somehow the bones in the feet must have also gotten larger, most likely from periosteal growth by the irregular bones in the feet, pushing the long bones in the toe region outwards.
Process #2
What we just proposed, which is that the pelvic bone structure was slightly rearranged, with all 3 main joints become looser. The symphysis pubis increases to 5 mm, but in some bone disorders, it becomes stretched to as much as 2 cm. The sacroiliac joints, which have articular cartilage on the sacral bone surface and fibrocartilage on the iliac bone surface, sort of pops out a little, gaining a higher degree of movement, and range. The result is that from resting on her back, the pregnant women has the two wing-like bones on the sides lower themselves from the central vertebrate.
One of the most common problems during pregnancy is the pelvic girdle pain, where the joints become inflammed. This inflammation means that either one or both of the cartilage surface of the sacroiliac joint becomes thickened. Sure, the cartilage thickness is very , VERY small, at around just 1-2 mm. However, we find out that the cartilage thickness in women is slightly more than in men. The thickened cartilage, to maybe 5 mm or even 10 mm from inflammation due to pregnancy causes the lower body bones to be pushed downwards, thus increasing the overall height of the woman.
Process #3
Due to the release of relaxin, certain intervertebral discs and bones in the lower back and sacral vertebral area become slightly looser. The ligament relaxes, the discs swell up slightly, and the pregnant woman lieing down on her side in the fetal position, pops the intervertebral discs which are almost almost immobile to become mobile for the 9 and a half months when she is carrying the baby. When the pregnancy is over, the discs ossify again, but the change has been that the discs have become slightly thicker.
So the question one might ask is, why is this phenomena not seen more often?
We suspect that more often, pregnant women will actually loose height from their lower back region due to the discs being compressed by the extra weight of the baby.
We suspect that if a women can be induced to be in a constant pregnant state with the same level of hormones (O-estrogen, Progesterone, Follicle Stimulating Hormones, etc) going her body, however without the baby in the uterus, and we placed the woman in some type of spinal decompression machine, attached to her hip region and lower back, she can be stretched out to be 2-3 inches taller, and that height increase would be permanent.
We had proposed this idea that some people, women especially, may have never had their growth plates fused properly “A Theory That Epiphyseal Growth Plates Never Fuse For Certain People“
Just two weeks ago, a women messaged us telling us that even at the age of nearly 30 she found out from an X-ray done after a fall that her growth plates were open.

This phenomena is very common among certain women, and it is hard for us to explain.
The obvious explanation from a social perspective is that these women noticed that their height stopped increasing in their teens and assumed that their growth plates were gone and they won’t grow anymore. They never needed to get any type of X-ray to validate this idea since no-one has X-ray vision to confirm it. A growth plate is not something that you can see with the naked eye.
The best explanation from a mechanistic, molecular, or physiological POV is that the women had a weight and BMI which was much lower than average. The weight load on the growth plates never reached a level to fully ossify the rest of it.
We refer to the PubMed study “Fundamental limits on longitudinal bone growth: growth plate senescence and epiphyseal fusion“.
In the study, it was found that as a person’s weight increases, the weight actually forces the chondrocytes in the resting zone to be used up.
The rate of the depletion of the MSCs that differentiate into the chondrogenic lineage from the resting zone is dependent on the weight on top of the tibia bone (or any bone that contributes to the overall height). Gravity is the force forcing the chondrocytes to be used up.
Mathematically, this phenomena can be described as a type of differential equation.
(alpha)*(-dCh/dt) = W & at t(time) = o , Ch = Constant # of Chondrocytes in resting zone (We are also assuming that the initial number of chondrocytes does not get replenished.) W= weight,
However W = beta*rho*(dCh/dt)^3 (or 3/2)
The need to use a power of 3 (or maybe a 3/2) is due to the fact that a dCh/dt leads to a delH or change in height, which is just 1 dimensional. However, the weight is determined by volume, which is 3 dimensioned, based on W=rho*V where rho is the density of the body. and V=L^3 and dCh/dt=gamma*dL
As long as a person does not go over a certain weight in their torso, the cartilage does not become completely ossified. However, once the person gains too much weight on their upper body, the growth plates are used up.
This would explain our hypothesis that certain people, but especially women, have some epiphyseal cartilage left which was never used up. They never got heavy enough.
We suspect that the type of women who would have this happen are girls who went through anorexia or dieted in the extreme. The low weight and their stunted growth (due to not eating right) would cause the senescence of the growth plates to be arrested. Once they get over the anorexia, maybe in their 20s or even late 20s, the cartilage gets reactivated, and the cartilage goes into catch-up growth. Of course, all of this is just our best guess at this point.
Main Takeaway
A small percentage of women, most likely thin girls during their teenage years, will notice a 1-3 inch of height gain from them going through pregnancy.