Update August 1st, 2013: The conversation on this issue on whether inhibition of FGFR3 between Me and Raj continue with the following messages…
Raj —> Me
Unfortunately Michael, I don’t think you really got the point of my message.
You state: “We can not translate the chondrocyte dysplasia of rats to humans. The first reason is that dysplasia does not always equate to hyperplasia. The growth plates may go through dysplasia but that usually means that the subject is going to develop stunted growth instead of increased growth.”
In the two studies you looked at, about PD176076, it states that mice did have increased growth plate height, but with overall dysplasia. The dysplasia is caused by PD176076’s effect as a VEFGR inhibitor as well.
My point was that if FGFR3 inhibition will lead to hyperplasia, but ONLY if we target FGFR3, not VEGFR. The problem with current pharmaceuticals are the lack of specificity between different tyrosine kinases. As the study above states, PD176076 is also a VEGFR inhibitor. Inhibition of VEGFR will in fact lead to stunted growth (google this). Please, do some more research. Look at case studies were scientists have examined families with mutations in FGFR3. These people have tall stature caused by the hyperplasia of the growth plates.
But you are right, it does not say anything about the regeneration of growth plates. I specifically stated in my first message that this could be effective for individuals whose growths had just recently closed.
Again, you need to do more research.
Me —> Raj
so how would the inhibition of FGFR3 and the prevention of the inhibition of VEGFR help a person who recently had their plates fused? I am already doing research on something else. help out.
take a look at calves with spider lamb syndrome. Their legs may be longer, but the limb will be bent/crooked.
Raj —> Me
Spider legs – a developmental defect.
Even if it does lead to spider legs, it should return to normal because our genes weren’t designed to cause spider legs.
And yeah, I’ll get cracking on that.
Most of the comments and emails I get to the website are not very helpful in the research. However, sometimes someone makes a comment or references of a study which causes a big change in our research. It seems that just recently a person named Raja wrote a comment stating that it might be possible for people who have had their growth plate close recently to reopen new plates slightly by inhibiting one of the Fibroblast Growth Factors, FGF3.
The Original Comment…
Growth plate regeneration may actually be possible for people between 17-21. Inhibition of FGFR3 may restore the growth plate, by a very small degree, as stated in the paper here: http://tpx.sagepub.com/content/33/4/449.abstract. If we can regenerate the growth plate using FGFR3 inhibitors, we can use other kinase inhibitors (or pharmaceuticals) to increase the height of the growth plate, which can potentially increase final height as well. I am currently researching pharmaceuticals to achieve this and how to synthesis different FGFR3 inhibitors. Also, it has been PROVEN that FGFR3 inhibition causes skeletal overgrowth (just google this).
{Tyler’s Comments in Italics+Bold}
The Study – Cartilage Dysplasia and Tissue Mineralization in the Rat Following Administration of a FGF Receptor Tyrosine Kinase Inhibitor
Abstract – PD176067 is a reversible and selective inhibitor of fibroblast growth factor receptor tyrosine kinase, and was in preclinical development as an angiogenesis inhibitor for the treatment of solid tumors. A 14-day oral toxicity study of PD176067 in young female rats (7 weeks old) was conducted at doses of 2.5, 5, and 10 mg/kg/day (15, 30, and 60 mg/m2, respectively). Skeletal changes, and vascular and soft tissue mineralization were observed as primary drug-related toxicities. To determine if these changes are specific to young, rapidly growing animals with increased vascular and osseous development, PD176067 was administered to mature (11 months old) rats. Female rats received PD176067 by gavage for 14 days at doses of 2.5, 5, and 10 mg/kg/day and necropsied on day 15. Clinical signs of toxicity were seen at ≥5 mg/kg and one death occurred at 10 mg/kg. Physeal dysplasia{physeal dysplasia means that the growth plate grew and should result in longitudinal bone growth; 11 month old rats are pretty much growth plate senescent} (distal femur, proximal tibia, sternum) occurred in all drug-treated animals and was characterized by dose-related increased thickness of the zones of chondrocyte proliferation and hypertrophy, and marked thickening of the zone of ossification. Cartilage hyperplasia was characterized by proliferation of chondrocytes along margins of the synchondrosis and subperiosteum of sternebrae{if the origin of the growth plate chondrocytes was periosteum then it would mean that this FGFR1 inhibition could work on people without growth plates as older individuals could merely acquire new growth plates via the periosteum}. Serum phosphorus levels increased 47% and 166% at 5 and 10 mg/kg, respectively. Mineralization of cardiac myocytes, aorta, various arteries, renal tubules, and gastric mucosa and muscularis was seen at 10 mg/kg, and consistent with the presence of calcium-phosphorus deposition. Physeal changes occurred at similar plasma PD176067 exposures in young and mature rats (AUC ≥ 4.83 μg · hr/mL). PD176067 produced morphologically similar lesions in young and adult rats.
Initial Analysis – From doing only a reading of the abstract it seems that if we give this type of selective inhibitor of fibroblast growth factor receptor tyrosine kinase known as PD176067 to lab rats, the physis (growth plates) in its limbs goes through dysplasia. In the experiment, the lab rats were used to test the toxicity of the compound. Different dosages were used and young and old rats were tested. What is seen is that the zones of the growth plates did increase in thickness. There was signs of cartilage hyperplasia where the chondrocytes on the edges of the articular and epiphyseal cartilages replicated much faster. What is not good is that something else known as serum phosphorous increased. The bigger problem is that parts of the heart, aorta, and various arteries started to become mineralized. The effects were very similar in both the young and old rats.
From reading only the abstract I conclude that while it might be that this specific FGF receptor tyrosine kinase can cause the cartilage in joints to go through abnormal development and get thicker, there is no evidence that administering of any type of inhibitor of FGFR3 would lead to the reappareance of growth plates that might have been recently ossified.
Since Raja did say that I can just google the information about the link between inihibition of FGF3 and skeletal overgrowth, I did just that. The results are in the Further Research subsection
Deeper Analysis from Reading the Full Study PDF HERE – The first thing that is noted is that researchers have discovered that it is possible to stop cancer tumors from getting bigger by restricting the angiogenesis aka creation of blood flow to the tumor. Compounds like VEGF and FGFs actually can bind to receptors on cell surfaces with tyrosine kinase activity.
From the article “PD176067 is a reversible, selective ATP competitive inhibitor of FGF receptor tyrosine kinase, with in vitro IC50 values of 2–9 nM against human FGF receptor-1 (Parke-Davis, 2000)….inhibition of VEGF receptor tyrosine kinase is also observed, although at higher concentrations than for FGF receptor tyrosine kinase.”
The thing is that the researchers wanted to test just how toxic this inhibitor of FGF can be, young rats around 7 weeks old got various dosages twice a day. The result is that the growth plate in the young rats started to develop abnormally. In addition, many of the soft tissues started to mineralize and blood vessels also started to mineralize.
The section that would be most important to either validate or disprove the claim made by the commenter Raja that administering of a FGF Receptor Inhibitor is the section below, which I copy and pasted from the discussion section.
Abnormal endochondral ossification induced by PD176067 and classified as physeal dysplasia was present in the distal femur and proximal tibia growth plates in young rats at ≥5 mg/kg and mature rats at all doses. In young rats, progressive thickening of the physis was dose-related and severity of physeal dysplasia was minimal, mild, and mild to moderate at 2.5, 5, and 10 mg/kg, respectively. There was an approximately 4-fold increased thickness of cartilaginous growth plates in young rats at 10 mg/kg compared to agematched controls{That could be a pretty big increase in height} (Figure 3A and 3C). In young rats, the proliferating zone had increased numbers of flattened chondrocytes aligned in columns and was twice the thickness as compared to control rats{The increased number of flattened chondrocytes could be due FGFR1 resulting in disorganized flattened growth plates or it could be that FGFR1 inhibition results in chondrogenesis of subperiosteal cells resulting in possible new growth plate formation}. There was increased depth of the zone of chondrocyte hypertrophy, and marked thickening of the zone of ossification (primary spongiosa). Disorganization of the distal columns of hypertrophic chondrocytes, variable enlargement of the perichondrial lacunae, and increased numbers of primary spongiosa with retention of cartilaginous cores and thin rims of osteoid lining the trabeculae were present (Figure 3C). Capillary loops were present within the tubes of mineralized cartilage matrix (Figure 3E). However, there was decreased resorption or amalgamation of primary spongiosa into secondary spongiosa.
In mature control rats, the narrow, inactive physes were sealed by a layer of bone along the zone of ossification, and the metaphyses contained a few thick trabeculae (Figure 3B). With administration of PD176067 to mature rats, there was enhanced proliferation and maturation of chondrocytes. There was increased prominence of the stacks of proliferating chondrocytes and an approximately 2-fold increased thickness of the zone of hypertrophy (Figure 3D). The metaphysis contained irregular thick trabeculae with retention of chondrocytes and cartilage cores (Figure 3F).
In both young and mature rats, the synchondroses of sternebrae were thickened by proliferating and hypertrophic chondrocytes (Figure 4A, 4B, and 4C). The cartilage hyperplasia elevated and extended along subperiosteal margins of the sternebral body with resemblance to endochondral ossification in young rats.
From the Results Section
Oral administration to rats of an inhibitor of VEGF receptor tyrosine kinase (AstraZeneca’s ZD4190) resulted in a marked increase in the femoral physeal zone of hypertrophy (Wedge et al., 2000). Administration of a recombinant humanized anti-VEGF monoclonal IgG antibody (rhuMabVEGF) to young adult cynomolgus monkeys produced physeal dysplasia characterized by increased hypertrophied chondrocytes, subchondral bony plate formation, and inhibition of vascular invasion of the growth plate (Ryan et al., 1999).
Deletion of the murine FGF receptor-3 gene resulted in mice (FGFR-3−/−) that developed bone dysplasia characterized by expansion of proliferating and hypertrophic chondrocytes within the growth plate (Deng et al., 1996). The study by Deng et al. suggested that FGF receptor-3 regulates endochondral ossification by limiting chondrocyte proliferation in the growth plate; therefore, inhibition of receptor function results in chondrocyte proliferation.
PD176067 administration to rats resulted in chondrocyte proliferation and cartilage formation, characterized by increased thickness of both the zone of proliferation and the zone of hypertrophy. Although the mechanism by which this occurs in rats is unknown, inhibition of FGF and/or VEGF
dependent signaling pathways appears to be a component. In summary, the current and published data suggest that inhibition of growth factor signaling can lead to increases in chondrocyte proliferation and expansion of the hypertrophic zone, resulting in dysplastic growth of cartilage
From the Discussion Section
In conclusion, oral administration of PD176067 to female rats for 14 days resulted in physeal dysplasia and soft tissue mineralization. These lesions were morphologically similar in young and mature rats, and do not appear to be related to inhibition of angiogenesis. Tissue mineralization was associated with elevated serum phosphorus levels and was consistent with calcium phosphorus deposits.
Personal Conclusion – When I only analyze this specific type of FGF inhibitor, it shows that it can cause many sections of the growth plates in at least young rats to become expanded in thickness. When it is applied to older rats, who actually still have cartilage in their limb bones, the researchers write “With administration of PD176067 to mature rats, there was enhanced proliferation and maturation of chondrocytes. There was increased prominence of the stacks of proliferating chondrocytes and an approximately 2-fold increased thickness of the zone of hypertrophy“
Now, let’s always remember that even in mature rats which might be many months old and don’t get their limbs growing longitudinally longer, their limbs are still cartilage tissue. When the researchers are saying that the chondrocytes did proliferate in mature rats, it is more likely that they are referring to the fact that mature rats still have chondrocytes in their long bones since the long bone still has cartilage in them. It seems that the growth plate never goes away for lab rats{The growth plate is still dysfunctional in older rats such that longitudinal bone growth stops so it is promising that growth begins a new; one possible method for growth beginning anew is the accumulation of new growth plate cells from the periosteal region which could potentially happen in older adults}. When the researchers are talking about the zone of hypertrophy in mature rats, that is what they are talking about.
Overall, after even read the entire PDF for the full study, there is no evidence that there can be growth plates can be be restored even slightly for humans. The reason is because old rats have cartilage in their long bones, and humans do not. We can not translate the chondrocyte dysplasia of rats to humans. The first reason is that dysplasia does not always equate to hyperplasia. The growth plates may go through dysplasia but that usually means that the subject is going to develop stunted growth instead of increased growth{While true that skeletal dysplasia doesn’t always result in increased height, it seems however that dysplasia’s relating to FGFR3 inhibition and/or CNP stimulation uniformly result in increased longitudinal bone growth, although in this study FGFR1 is inhibited and not FGFR3}.
I would say that the suggestion made by the commenter Raja is inaccurate and was a too big of a leap in scientific reasoning and logic. The studies never stated directly or implied that it would work in adult humans.
Tyler’s Comments:
It’s interesting that PD176067 is actually an FGFR1 and VEGFR2 inhibitor and not an FGFR3 inhibitor when FGFR1 is typically considered the good FGFR and FGFR3 the bad. It should be noted that LSJL does result in upregulation of FGFR1 mRNA. FGFR1 is involved in the commitment of stem cells to chondrocytes. Maybe only downregulation of beta-catenin is required to commit stem cells to chondrocytes and FGFR1 merely plays an inhibitory role.
As a result of the FGFR1 inhibitor treatment there was increased incidence of hypocellularity bone marrow lesions(fewer cells than there should be) with increasing dose and increasing age. It’s possible that the fewer cells are a result of these cells being used as growth plate cells.
As a result of FGFR1 inhibition there was also ectopic mineralization in the heart, kidneys, stomach, and arteries. This could be the result of ectopic endochondral ossification in those areas thus the possibility that FGFR1 inhibition could in fact help form new growth plates. It’s possible though that the ectopic mineralization is as a result of dysregulation of phosphorus and calcium as suggested in the study.
 A, C, and E are from young growth plates whereas A, D, and F are from mature growth plates.
A, C, and E are from young growth plates whereas A, D, and F are from mature growth plates.
“Growth plate of mature control rat is inactive and sealed by layer of bone (arrow).”<-so FGFR1 inhibition could possibly “unseal” the bone.
I also found another study which likes FGFR3 to BMP Type 1 receptor which is highly significant as BMPR1A may play a role in growth plate formation.
FGFR3 induces degradation of BMP type I receptor to regulate skeletal development.
“chondrocyte-specific deletion of BMP type I receptor a (Bmpr1a) rescued the bone overgrowth phenotype observed in Fgfr3 deficient mice by reducing chondrocyte differentiation{for our purposes Bone overgrowth is a good thing}. FGFR3 inhibited BMPR1a-mediated chondrogenic differentiation. FGFR3 hyper-activation resulted in impaired BMP signaling in chondrocytes of mouse growth plates. FGFR3 inhibited BMP-2- or constitutively activated BMPR1-induced phosphorylation of Smads through a mechanism independent of its tyrosine kinase activity. FGFR3 facilitate BMPR1a to degradation through Smurf1-mediated ubiquitination pathway. Down-regulation of BMP signaling by BMPR1 inhibitor dorsomorphin led to the retardation of chondrogenic differentiation, which mimicks the effect of FGF-2 on chondrocytes and BMP-2 treatment partially rescued the retarded growth of cultured bone rudiments from thanatophoric dysplasia type II mice.”
“BMP-2 significantly promoted the hypertrophic zone length of embryonic metatarsals, but not the mineralized and proliferation zone length”
“Double Bmpr1a and Bmpr1b null mice have a phenotype of increased expression of FGFR1 in chondrocytes”
Thus inducing BMPr1a expression in stem cells could possibly aide in inducing neo growth plate formation.——————————————–
Further Research – I did google the term and the following studies were listed and I did read over the abstracts of these studies
Study #1: Fibroblast growth factor receptor 3 effects on proliferation and telomerase activity in sheep growth plate chondrocytes
Personal Interpretation – Researchers are in agreement that FGFR3 causes chondrocytes in growth plates to decrease in proliferation. It causes the decrease through down-regulating TERT expression and reducing telomerase activity indicating an important role for telomerase in sustaining chondrocyte proliferative capacity during bone elongation. From the researchers “The present study addressed whether reduced FGFR3 expression enhanced telomerase activity, mRNA expression of telomerase reverse transcriptase (TERT) and RNA component of telomerase (TR), and chondrocyte proliferation, and whether the stimulation of FGFR3 by T3 evoked the opposite response.”
Study #2: Enhanced skeletal growth of sheep heterozygous for an inactivated fibroblast growth factor receptor 3
Personal Interpretation – It seems that when the FGFR3 is inhibited in sheep, the condition is known as spider lamb syndrome. It was shown that lamb that had it, whether homozygous or heterozygous did end up with longer limbs and were taller than their counterparts. It did take longer for the lamb to reach the same weight as the normal ones but they did end up bigger in terms of the size/volume of the bones.
Study #3: Constitutive activation of MEK1 in chondrocytes causes Stat1-independent achondroplasia-like dwarfism and rescues the Fgfr 3-deficient mouse phenotype
From The Study – “the MAPK pathway inhibits hypertrophic differentiation of chondrocytes and negatively regulates bone growth without inhibiting chondrocyte proliferation. Expression of a constitutively active mutant of MEK1 in chondrocytes of Fgfr3-deficient mice inhibited skeletal overgrowth, strongly suggesting that regulation of bone growth by FGFR3 is mediated at least in part by the MAPK pathway…a model in which Fgfr3 signaling inhibits bone growth by inhibiting chondrocyte differentiation through the MAPK pathway and by inhibiting chondrocyte proliferation through Stat1…FGF receptor 3 (FGFR3) is expressed in proliferating and prehypertrophic chondrocytes in the epiphyseal growth plates.”
Study #4: A Lys644Glu Substitution in Fibroblast Growth Factor Receptor 3 (FGFR3) Causes Dwarfism in Mice by Activation of STATs and Ink4 Cell Cycle Inhibitors
Personal Interpretation – The researchers used genetic engineering to add a mutation into the chondrocytes of the growth plate in lab rats. The mutation is the substitution of something known as Lys644Glu. The result is increased FGFR3 expression, leading to mice that showed signs of dwarfism and small skeletal size.
Link #1: FGFR3 is a physiological negative regulator of bone growth
Link #2: Molecular mechanisms of FGFR3 signaling in cartilage
Related Information
It seems that for a long time there was a lot of studies which showed that this receptor for FGF3 have been very involved in skeletal growth.
Tyler wrote about the fact that FGFR3 was another idea that we should explore in an old post from backin October of 2011 entitled “FGFR3“. The most interesting thing that he showed was that there was some project by the NIH for a way to treat the stunted growth of FGFR3 using a soluble form of FGFR3 entitled “DELIVERY OF SOLUBLE FGFR3 AS A TREATMENT FOR ACHONDROPLASIA“. The author is Steve Ghivizzani, Ph.D. with the University of Florido, Department of Orthopaedics and Rehabilitation at the College of Medicine.
The grant proposal writer notes that achondroplasia is almost always caused by the excess expression of FGFR3. They propose this idea to remove the stunting of growth due to excess FGFR3. “we hypothesized that systemic delivery of a soluble FGFR3 molecule would likewise titrate receptor-specific FGF ligands and thereby reduce aberrant FGFR3 signaling to rescue bone growth….We will address the following Specific Aims:
- To determine the capacity of FGFR3?TM to bind FGF-ligand and thereby inhibit aberrant FGFR3G374R signaling in growth plate chondrocytes from transgenic and knock-in models of achondroplasia.
- To determine the effects of long-term delivery of FGFR3?TM on the skeletal growth and physiology of the FGR3G374R knock-in achondroplasia model.
On a related note on the subject of FGR3…
I was combing through the threads of the Make Me Taller boards and there was a post that noted that FGFR3 and the inhibition of it was one of the only ideas ever pursued by a real company to try to increase growth and height in humans. From the thread “Starting up a biotech research/investment company” someone (Harald Oberlander) writes this part….
Worldwide there is currently very few research activity concerning new height increase / limb lengthening therapy options.
Children: To the best of our knowledge there is currently only one company worldwide, that researches an innovative height increase therapy: ProChon Biotech (http://www.prochon.com), established in Israel in 1997. ProChon is developing a monoclonal antibody for the treatment of achondroplasia. This antibody approach targets specifially the FGFR3-gene and hasn´t reached the stage of human clinical trials yet. If it is successful, it will only work for children with achondroplasia.
The fact is that Harald specifically named the name of a company that has been doing research to figure out how to make children taller beyond the traditional GH therapy.
It is ProChon Biotech, and it was using the type of technology that Raja is proposing, which is to target/inhibit the FGFR3 gene.
I would go to the ProChon website and read up more about this company. It seems that the company was created to find ways to regrow or regenerate cartilage tissue. The focus was on tissue regenerative technologies to relieve pain in knees from regenerating articular cartilage. The product that was created by ProChon and sold was something called the BioCart™ Cartilage Regeneration System. The system was a technology created to heal articular cartilage defects through microfractures. It was eventually bought out through stock options in May of 2011 by the company Histogenics Corporation, which also was in the cartilage regeneration and repair field.
One of the members on the board I became very interested in reading more about in terms of the research and the paper they have written, a Dr. Avner Yayon. I would try to search any research papers he had written in PubMed by typing in his name Avner Yayon. His papers may help further the research and might give a clue which direction the research should be going towards.
Conclusion – This shows that for children with growth plates at least, the possibility of increasing height is very likely using this other method, by finding a way to inhibit this specific FGF.

 I was recently listening to this episode where a person went on the radio to talk about how the late Nikola Tesla proclaimed that most of the universe’s hidden secrets can be found if a person would approach his analysis through the lens of looking at the world from a perspective of it being electromagnetic stimuli, energy, frequencies, and vibrations. The most famous quote to this claim was “If you want to find the secrets of the universe, think in terms of energy, frequency and vibration” – Nikola Tesla.
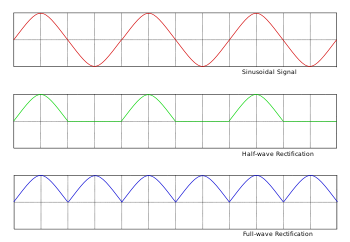
I was recently listening to this episode where a person went on the radio to talk about how the late Nikola Tesla proclaimed that most of the universe’s hidden secrets can be found if a person would approach his analysis through the lens of looking at the world from a perspective of it being electromagnetic stimuli, energy, frequencies, and vibrations. The most famous quote to this claim was “If you want to find the secrets of the universe, think in terms of energy, frequency and vibration” – Nikola Tesla. I had previous showed that it might be possible to induce the bones to increase the rate of endochondral ossification with something as simple as a Function Generator or even a TENS Unit which often cost less than $100.
I had previous showed that it might be possible to induce the bones to increase the rate of endochondral ossification with something as simple as a Function Generator or even a TENS Unit which often cost less than $100.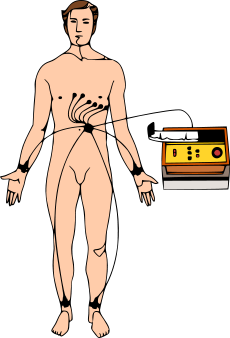 The heart operates actually on a very clear rhythm of electrical signal. For the people who have ever had an ECG (Electrocardiography) done, they have probably been told that what is being measured is the electrical signal that is coming from the heart beating. If there is some type of irregularity in the heartbeats, this is known as arrhythmia. To correct for it most people get some type of internal Implantable Cardioverter Defibrillator. If however the person is already on the ground, most emergency rescue personnel with some type of advanced life support (ALS) or basic life support training (BLS) will use some type of portable external defibrillators to reset the rhythm of the heart beating. What we are trying to say is that at the most basic level, our most important internal organs, the brain and heart, both operate on electrical current.
The heart operates actually on a very clear rhythm of electrical signal. For the people who have ever had an ECG (Electrocardiography) done, they have probably been told that what is being measured is the electrical signal that is coming from the heart beating. If there is some type of irregularity in the heartbeats, this is known as arrhythmia. To correct for it most people get some type of internal Implantable Cardioverter Defibrillator. If however the person is already on the ground, most emergency rescue personnel with some type of advanced life support (ALS) or basic life support training (BLS) will use some type of portable external defibrillators to reset the rhythm of the heart beating. What we are trying to say is that at the most basic level, our most important internal organs, the brain and heart, both operate on electrical current.