
With my latest focus on research and experimentation of torsion leading potential bone overgrowth(new longitudinal bone growth). I did some research on scoliosis as in scoliosis there is a lot of research on the spine. Therefore, if torsion could stimulate longitudinal bone growth we’d expect to see overgrowth of the spinal column. It may still be possible however that even if scoliosis did not increase longitudinal bone growth that torsion may still increase longitudinal bone growth as scoliosis may not meet the dynamic threshold over which torsion stimulates longitudinal bone growth. However, I think the papers do suggest that scoliosis causes bone overgrowth.
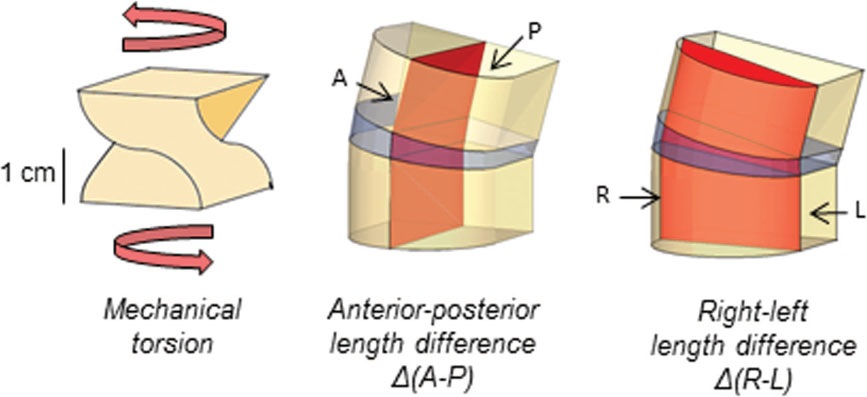
“High-resolution computed tomographic scans of 77 patients with severe adolescent idiopathic scoliosis were included. Torsion and anterior-posterior and right-left asymmetry of each individual vertebral body and intervertebral disc were studied from T2 to L5, using semiautomatic analysis software. True transverse sections were reconstructed along the anterior-posterior and right-left axis of all endplates. These “endplate-vectors” were calculated semiautomatically, taking rotation and tilt into account. Torsion was defined as the difference in axial rotation between 2 subsequent endplates. Asymmetry was defined as the relative anterior-posterior or right-left height difference of the discs and the vertebrae.”
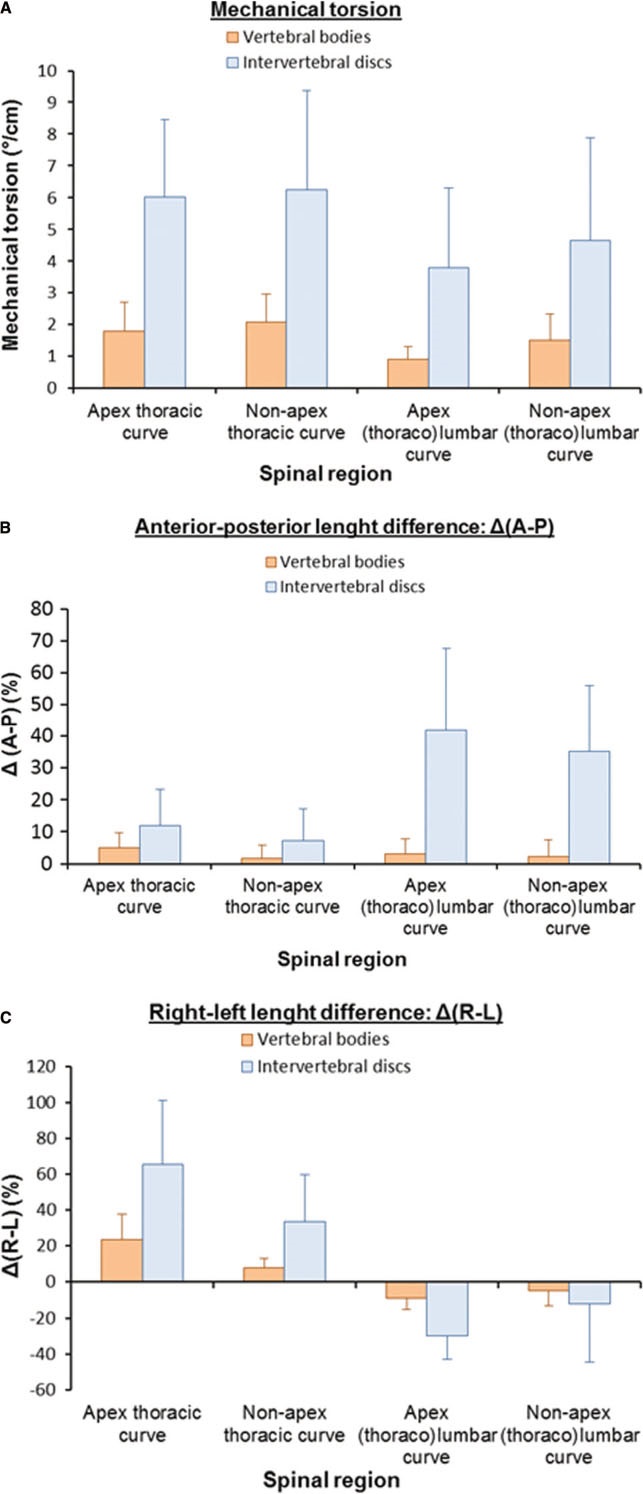
“There were at least 3 times more torsion, anterior overgrowth, and coronal wedging in the discs than in the vertebrae in the thoracic as well as in the (thoraco) lumbar curves (P < 0.001). These values correlated significantly with the Cobb angle (r ≥ 0.37; P < 0.001). Anterior overgrowth and coronal asymmetry were greater in the apical regions whereas torsion was most pronounced in the transitional segments between the curves.”<-just because torsion is more pronounced in certain segments does not mean that other segments did not undergo torsion overall.
“The discs contribute more to 3-D deformity than the bony structures, and there is significant regional variability. This suggests an adaptive rather than an active phenomenon.”<-the adaptative phenomenon could be torsion.
“On conventional 2-dimensional radiographs, it was observed that the discs were more wedge-shaped than the vertebral bodies in mild scoliotic curves whereas the wedging of the discs and vertebrae became more or less equal in more severe scolioses. These findings suggest that AIS[adolescent idiophatic scoliosisi] is primarily a deformation of the discs and that, according to Hueter-Volkmann’s law[compressed growth plates grow less, stretched growth plates grow more], the deformation of the vertebral bodies is secondary. However, at the same time, others reported increased coronal wedge angles of the vertebral bodies already in mild AIS, indicating abnormal vertebral growth.”
“Torsion per centimeter height: This was defined as the angle between the anterior-posterior axis of the superior endplate and the anterior-posterior axis of the inferior one of the same vertebra or disc in the axial plane divided by the height in centimeters. For example, if we found 3 vertebrae with a total height of 6.0 cm and a total torsion of 15°, torsion was 2.5°/cm.”
” all individual AIS curves were longer anteriorly than posteriorly and rotated both between and within vertebrae in the axial plane. This rotated lordosis has been described by a number of authors, leading to the hypothesis that lordosis is the initiating deformity, and that scoliosis is the result of a disturbed anterior versus posterior growth process”
“anterior “overgrowth” of the discs versus vertebrae in the sagittal plane”
“These findings support that AIS is mainly a 3-D deformity of the discs, suggesting that abnormal vertebral growth is, according to Hueter-Volkmann’s law, rather a consequence than a cause of the deformity”
“scoliosis as a rotatory instability of the spine, and the development of AIS depends on disturbance of the delicate balance between rotational stiffness of the spine on the one hand and rotation-inducing forces on the other. Once the spine decompensates into rotation around the stiff posteriorly located ligamentous axis, the vertebral bodies swing farther away from the midline than the posterior structures. At that point by definition, a lordosis starts to develop, leading to greater anterior length of the spine.”
“In conclusion, the IVDs contribute more to the 3-D deformity in AIS than the vertebral bodies. Because the processes of torsional deformation, anterior overgrowth, and coronal wedging are greater in the discs than in the vertebral bodies and are uniform in primary as well as compensatory AIS curves, it seems more logical that these morphological modifications are rather a consequence (among others through Hueter-Volkmann’s law) than a cause of the deformity.”<-so this suggests that torsion could potentially cause overgrowth.
Since scoliosis can be altered through exercise as suggested by studies such as Scoliosis-Specific exercises can reduce the progression of severe curves in adult idiopathic scoliosis: a long-term cohort study, this suggests that mechanical loading via exercise can alter the discs and vertebral bodies in the same way that scoliosis alters the mechanical loading of discs and vertebral bodies and alters their shape. IN the paper it suggests that the reduction may be due to “concave ligament stretching.” The authors of this study refuse to indulge the possibility that the change may be due to reduction in bon
Relative anterior spinal overgrowth in adolescent idiopathic scoliosis deformity.
“. The differential growth between the anterior and the posterior elements of each thoracic vertebra in the patients with AIS was significantly different from that in the controls (p < 0.01). There was also a significant positive correlation between the scoliosis severity score and the ratio of differential growth between the anterior and posterior columns for each thoracic vertebra (p < 0.01). Compared with age-matched controls, the longitudinal growth of the vertebral bodies in patients with AIS is disproportionate and faster and mainly occurs by endochondral ossification. In contrast, the circumferential growth by membranous ossification is slower in both the vertebral bodies and pedicles”<-the faster growth could be due to mechanical stimulation by torsion.
“Relative anterior spinal overgrowth in AIS has been reported in morphological studies”
Here’s what’s meant by anterior:
“
The longitudinal growth of the anterior column occurs at the growth plates by endochondral ossification and continues until the girl is between 16 and 18 years of age. In contrast, endochondral ossification of the posterior elements is complete by the end of the first decade of life”
“The posterior elements subsequently only grow circumferentially by membranous ossification. We speculated that the pathomechanism of the disproportionate spinal growth in AIS might be a loss of coupling between endochondral and membranous ossification during adolescence.”
“the relatively shorter posterior column acts as a tether which hinders the lengthening of the anterior column during the period of rapid growth, forcing the spine to bend and rotate. Different tissues such as
bone, spinal cord, ligaments, and muscles are included in the posterior column. The issue is which structure in the posterior column causes the tethering.”
“Tethering of the posterior soft tissues such as the posterior ligaments has been presumed to
be the force acting on the spine to create the complicated deformity”<-I have seen other people theorize that the ligaments constrain longitudinal bone growth.
“There is much indirect evidence supporting the hypothesis that uncoupled endochondral-membranous bone formation causes the relative anterior spinal overgrowth in AIS. It is well known that girls with AIS have a tendency to be taller and thinner than their peers.”<-it is also possible that the scoliosis causes the overgrowth itself via torsional mechanical loading.
so this study suggests an alternative mechanism than torsion to cause the overgrowth but it does not rule out the torsion.